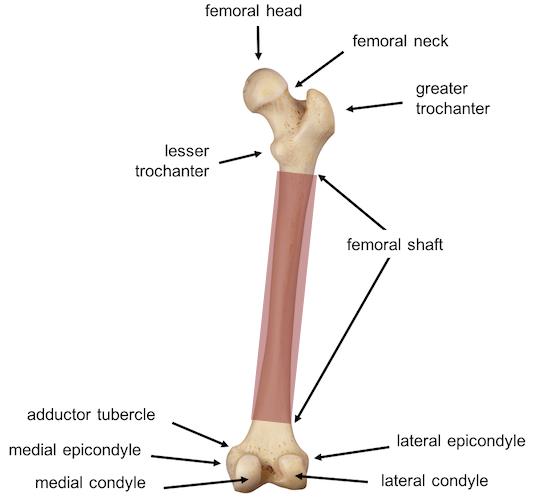
Femur Anatomy
Definition: Fracture of the femoral diaphysis between the area 5 cm distal to the lesser trochanter and 5 cm proximal to the adductor tubercle
Mechanism
- Direct Trauma: Motor vehicle collision, fall, child abuse
- Indirect Trauma: Rotational injury
- Pathologic Fracture: Secondary to osteogenesis imperfecta, tumors, bone cysts, non-ossifying fibromas
Epidemiology
- Bimodal distribution: Peaks from age 2 to 4 and again in mid-adolescence
- In children too young to walk, 80% are caused by child abuse
- Male predominance: 2.6:1
Physical Exam
- Inability to ambulate, extreme pain, tenderness to palpation (Eiff 2018)
- Thigh swelling and gross deformity common but not universally present
- Arterial Injury: distal paresthesias, diminished pulses
- Compartment syndrome: distal paresthesias, diminished pulses, distal weakness, pain with passive range of motion
Classification
- Descriptive (Egol 2010)
- Skin: open vs closed
- Level of fracture: proximal, middle, distal third
- Fracture pattern: transverse, spiral, oblique, butterfly fragment
- Comminution
- Displacement
- Angulation
- Anatomic
- Subtrochanteric
- Shaft
- Supracondylar
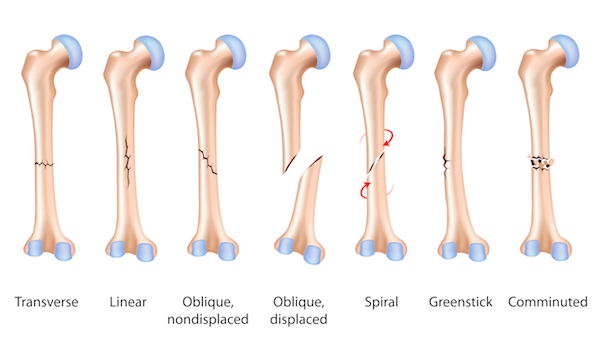
Femoral Shaft Fracture Classification (pathologies.lexmedicus.com)
 Imaging
Imaging
- Views
- AP and lateral femur XR
- Ipsilateral hip and knee XR to rule out associated injuries
- CT or MRI
- Generally unnecessary in acute management
- Consider to rule out associated femoral neck or acetabulum fracture
- Consider skeletal survey and head CT in infants with suspected non accidental trauma
ED Management
- In patients with a high energy mechanism of injury, start with a full head-to-toe trauma evaluation
- Remove any splints or bandages placed in the field and examine the overlying soft tissue to rule out open fractures
- Open fractures should be given antibiotics and tetanus booster
- Perform a complete neurovascular exam
- Pain management
- Systemic analgesics
- Femoral nerve blockuee
- Immobilization with splinting and/or traction can provide significant analgesia
- Orthopedic consult or transfer
- Always consider non accidental trauma in young children, consult child abuse specialist and social work as needed
- Treatment depends on age, fracture pattern, location, soft tissue trauma, and associated injuries; the American Academy of Orthopedic Surgeons summary recommendation
|
Age |
Treatment Options |
|
≤6 months |
Pavlik harness or Immediate spica cast |
|
6 months – 5 years |
Immediate spica cast or Traction → spica cast |
|
5 years – 11 years |
Flexible intramedullary nailing or Immediate spica cast |
|
11 years – maturity |
Rigid intrameddulary nailing or Submuscular/open plating or Flexible intramedullary nail (if <50 kg) |
Prognosis
- Children have a rapid and high rate of remodeling and few complications. As children get older their rates or remodeling decrease. .
- Potential complications include: leg length discrepancy (shortening or overgrowth), muscle weakness, osteonecrosis, malunion, and rarely nonunion
Take Home Points
- Do a full trauma exam on patients with femur fractures. Often, the injury occurs with a high energy mechanism and is associated with other injuries
- Consider non accidental trauma in children under 3 with this fracture pattern
- Provide early immobilization and orthopedic consultation
References
Anglen JO, Choi L. Treatment options in pediatric femoral shaft fractures. J Orthop Trauma. 2005; 19(10): 724-33. PMID: 16314721
Beaty JH, Kasser JR (Eds). Rockwood and Green’s Fractures in Children. Lippincott Williams & Wilkins, Philadelphia. 2010; 797 -841.
Cramer KE, Limbird TJ, Green NE. Open fractures of the diaphysis of the lower extremity in children. Treatment, results, and complications. J Bone Joint Surg Am. 1992; 74(2): 218-32. PMID: 1541616
Eiff MP, Hatch R. Femur and Pelvis Fractures: Femoral Shaft Fractures. Fracture Management for Primary Care. 3rd ed. Philadelphia: Elsevier Saunders. 2018; 221-224
Egol KA, Koval KJ, Zuckerman JD. Pediatric Femoral Shaft. Handbook of Fractures. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2010: 690-697
Flynn JM, Skaggs DL. Femoral shaft fractures. Rockwood and Wilkins’ Fractures in Children, 7th Ed.
Poolman RW, Kocher MS, Bhandari M. Pediatric femoral fractures: a systematic review of 2422 cases. J Orthop Trauma. 2006; 20(9): 648-54. PMID: 17088672
Kocher MS et al. Treatment of pediatric diaphyseal femur fractures. J Am Acad Ortho Surg. 2009; 17(11): 718 -25. PMID: 19880682
Heyworth BE et al. Management of pediatric diaphyseal femur fractures. Curr Rev Musculosketal Med. 2012; 5(2): 120-25. 22315162
Lewiss RE, Saul T, Shah KH. Femur Shaft Fracture. Essential Emergency Imaging. Philadephia: Lippincott Williams & Wilkins; 2012: 611-613
Madhuri V et alP. Interventions for treating femoral shaft fractures in children and adolescents. Cochrane Database Sys Rev. 2014; 29(7): CD009076. PMID: 25072888