This episode reviews the highlights from the recent ACEP clinical policy on acute VTE management in the ED.
Episode 148.0 – ACEP VTE Clinical Policy 2018

Show Notes
Take Home Points
- The PERC risk stratifies low risk PE patients (~10%) to a level low enough (1.9%) as to obviate the need for additional testing.
- Age-adjusted D-dimers are ready for use and it doesn’t matter if your assay uses FEU (cutoff 500) or DDU (cutoff 250). For FEU use an upper limit of 10 X age and for DDU use an upper limit of 5 X age.
- For now, subsegmental PEs should continue to routinely be anticoagulated even in the absence of a DVT. Keep an eye out for more research on this area.
- Although outpatient management of select PE patients (using sPESI or Hestia criteria) may be standard practice, the evidence wasn’t strong enough for ACEP to give it’s support
- Patients with DVT can be started on a NOAC and discharged from the ED
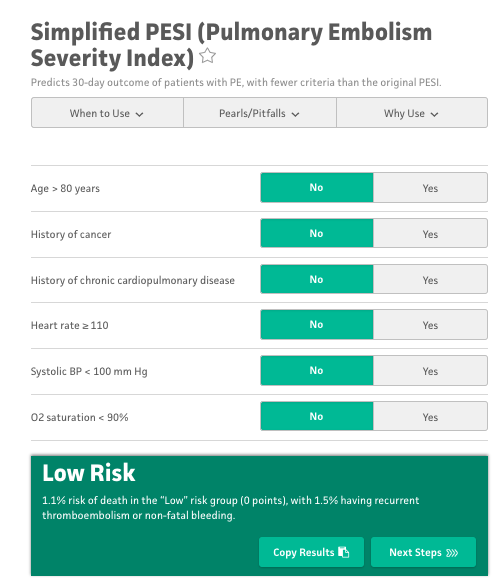
sPESI Tool (MDCalc.com)
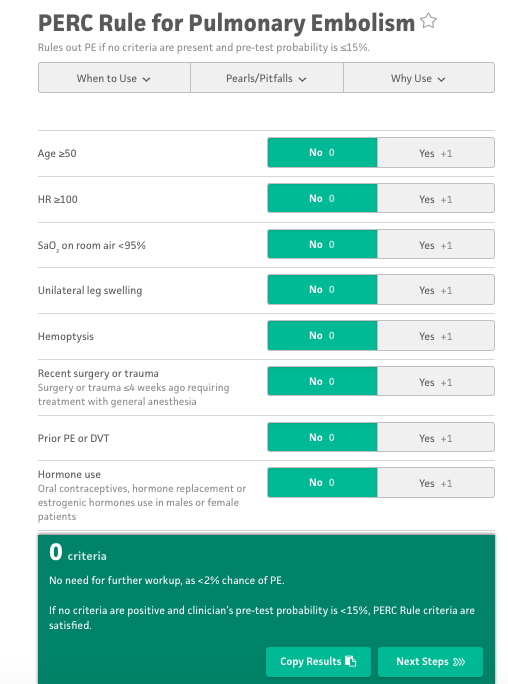
PERC Decision Tool (MDCalc.com)
Read More
- REBEL EM: ACEP Clinical Policy on Acute VTE 2018
- Core EM: PE Rule-Out Criteria RCT
- Core EM: Age-Adjusted D-dimer (Using D-dimer Units)
- Core EM: Age Adjusted D-dimer in PE – The ADJUST-PE Trial
- REBEL EM: Is It PROER to PERC It Up
References
- ACEP Clinical Policies Subcommittee. Clinical Policy: Critical Issues in the Evaluation and Management of Adult Patients Presenting to the Emergency Department with Suspected Acute Venous Thromboembolic Disease. Ann Emerg Med 2018; 71(5): e59-109. PMID: 29681319
- Jaconelli T, Eragat M, Crane S. Can an age-adjusted D-dimer level be adopted in managing venous thromboembolism in the emergency department? A retrospective cohort study. European journal of emergency medicine : official journal of the Eur Soc Emerg Med. 2017. PMID: 28079562
- Freund Y et al. Effect of the Pulmonary Embolism Rule-Out Criteria on Subsequent Thromboembolic Events Among Low-Risk Emergency Department Patients: The PROPER Randomized Clinical Trial. JAMA 2018; 319(6): 559-66. PMID: 29450523

