Background
A strategy of high-sensitivity cardiac troponins over short time intervals for the diagnosis of acute myocardial infarction has been recommended in European cardiology guidelines. It is unclear if the European strategy is generalizable to the US population. A strategy that identifies low risk patients early can lead to limited further diagnostic testing, ED length of stay, consultation and admission. This potential benefit should be compared to the potential risk of missed acute myocardial infarction.
Clinical Question
In US adults, presenting to the Emergency Department with a suspected non-ST elevation myocardial infarction, is a strategy using high sensitivity troponin over short testing intervals accurate in identifying those with and without acute myocardial infarction?
Design
Observational: Prospective Cohort
Population
- Inclusion: >22 years of age, presenting to the Emergency Department with suspected acute myocardial infarction for which a cardiac troponin level was sent
- Exclusion: STEMI
- Setting: US Multicenter (n=29): Mix of urban and community EDs. 4/2015-4/2016
Test
| 0 + 1 HOUR ALGORITHM | 0 + 2-3 HOUR ALGORITHM |
| Rule-Out Criteria | Rule-Out Criteria |
| 0-hour TPN < 3 ng/L OR | 0-hour TPN < 3 ng/L OR |
| 0-hour TPN < 6 ng/L + D TPN < 3 ng/L | 0-hour TPN < 8 ng/L + D TPN < 7 ng/L |
| Rule-In Criteria | Rule-In Criteria |
| 0-hour TPN ³ 120 ng/L OR | 0-hour TPN ³ 120 ng/L OR |
| Δ TPN >12 ng/L | Δ TPN >20 ng/L |
| Continued Observation | Continued observation |
| Not meeting rule-out or rule-in criteria | Not meeting rule-out or rule-in criteria |
| Levels at time 0, 45-90 minutes and 120-180 minutes
Troponin cutoff values were based on European algorithms Δ = Change between the 1st and 2nd samples |
|
Reference Standard
3rd Universal Definition of Acute Myocardial Infarction
Outcomes
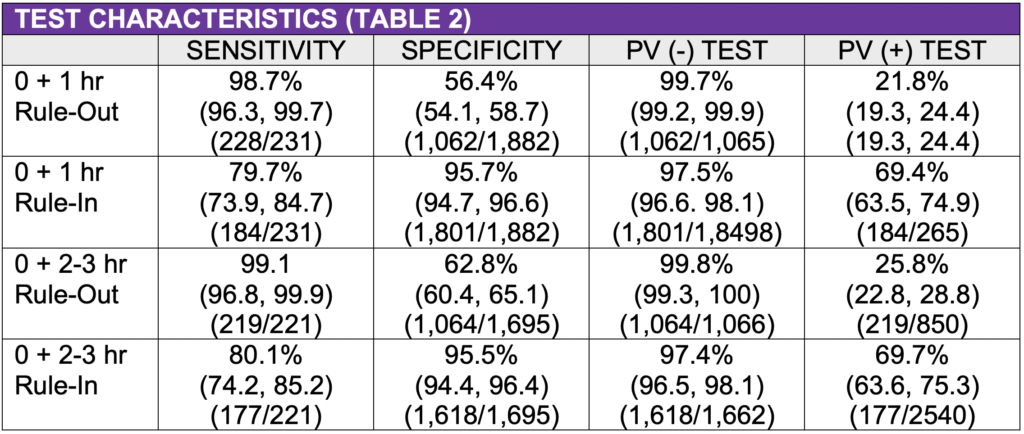
- Primary Outcome: Test Characteristics for Acute Myocardial Infarction (NSTEMI)
- Secondary Outcomes: 30-day Adverse Events:
- Mortality: All-cause, cardiac
- Non-fatal acute MI
- Coronary revascularization
- Heart failure
Primary Results
- n = 2,346 patients (0 + 1 hours: n = 2,113), (0 + 2-3 hours: n = 1,916)
- NSTEMI rate: 11.8% (278/2,346).
- Increased Risk: Male, ↑age, ↑number of risk factors, Hx coronary disease, abnl EKG, ↓renal function
- Both rule-out strategies had high predictive values of a negative test (0 + 1 hour: 99.7%, 95% CI (99.2, 99.9%), 0 + 2-3 hours: 99.8%, 95% CI (99.3, 100).
- 30-40% of patients not classified as rule in or rule out

Strengths
- Multicenter: n=29
- US mix of urban and community center
- Large sample (n=2,346)
- Improves generalizability
- Blinding: High SN troponin not available to treating clinicians or outcome assessors
- Well-defined reference standard evaluated by 5 MDs using all available data
- Included test characteristics as well as 30-day adverse events (99.5% follow up)
- Low risk of 30-day mortality/acute MI: 0+1hr = 0.2% (1 in 500), 0+2-3hr = 0.3% (1 in 333). Risk of adverse events increased: Rule Out < Continued obs < Ruled In)
Limitations
- Convenience sample potentially allowing for selection bias
- Repeat high-SN TPN not obtained on all: 1 (16%), 2 (40%), >3 (44%)
- Did not present breakdown of study population into risk groups (ruled out, out, ruled out or indeterminant) for comparison to algorithm risk assessment groups
- Test characteristics collapse 2 risk classification groups in one. For example, the 0 + 1-hour rule-out test characteristics compared patients who ruled-out to patients who did not rule-out. This includes patients who ruled-in and patients in the continued observation group).
- 30% unclassified as rule in or rule out
- High NSTEMI rate: 11.8%, populations with lower rates would have lower PV (-) test
- 30-day mortality and acute MI combined in K-M Curves. Not of equal importance
Author's Conclusions
“The accuracy for the early rule-out or rule-in of acute myocardial infarction with either a 0/1-hour or 0/2- to 3- hour novel high sensitivity cardiac troponin algorithm in a diverse US-based ED population is similar to that reported in comparable previous non-US studies, allowing a harmonization of these algorithms internationally. US ED patients can be equivalently evaluated with either a 0/1-hour or 0/2- to 3- hour algorithm. The rule-out zone high sensitivity cardiac troponin cut points of these algorithms additionally accurately predict the extremely low-prevalence 30-day outcomes of all-cause mortality and acute myocardial infarction, regardless of any ECG changes or the use of any clinical risk-stratification tools. The rapid rule-in of acute myocardial infarction with high sensitivity cardiac troponin assays requires more studies in the United States to improve the positive predictive values and specificities.”
Our Conclusions
This was a well-designed study with relatively minor validity concerns. The high sensitivity troponin algorithms demonstrated high negative predictive values for rule out criteria with a low risk of 30-day adverse events. However, 30-40% of patients did not meet rule in or rule our criteria.
Potential Impact To Current Practice
High sensitivity troponin has the possibility to rapidly exclude MI over short intervals but should be interpreted in the context of current risk stratification tools (e.g. HEART score) and EKG findings. A clinical decision rule incorporating all 3 factors would be helpful. The safety and efficacy of this approach needs to be compared to current risk stratification strategies.
Read More
REBEL EM: High Sensitivity Troponin Testing
