Background
Atrial fibrillation (AF) is one of the most common dysrhythmias encountered in the ED. Patients with chronic AF often present with increased heart rates, chest pain and weakness among other presentations. However, it’s the patients with new onset AF that really peak our interest. Why? Well, the management of these patients is potentially exciting, filled with procedures and clearly debatable.
The debate centers on whether patients with recent-onset AF should be rhythm controlled (e.g. converted back to sinus rhythm) or rate controlled only. This debate was showcased in a point-counterpoint in Annals of Emergency Medicine in 2011 (Stiell 2011, Decker 2011). The rhythm control supporters argue that AF is abnormal, worsens quality of life, leads to cardiac remodeling and, in may patients, requires medications for rate control and anticoagulation. The rate control group argues that cardioversion runs the risk of causing a thromboembolic event (i.e. CVA, peripheral arterial occlusion). Thus, it should not be performed until the absence of clot in the left atrium is confirmed (by TEE) or appropriate anticoagulation has occurred. It has long been taught that if the patient has been in AF for < 48 hours, the risk of developing a clot in the left atrium is negligible and cardioversion may be pursued. However, some recent literature has called this classic teaching into question (Nuotio 2014). Additionally, the rate control supporters argue that patients’ history may be unreliable in establishing time of onset.
Of note, most studies lump AF and atrial flutter together as the management and disposition is typically the same.
Clinical Question
What is the effectiveness and safety of a protocol to perform rapid cardioversion and discharge of patients who present with atrial fibrillation and flutter these?
Population
660 adult patients presenting with atrial fibrillation to a single hospital in Ottawa with symptoms of < 48 hours in duration.
Intervention
Ottawa Aggressive Protocol (see Box 1 of article) Basically, rate control if very symptomatic or not being cardioverted. Otherwise, procainamide infusion 1 gram over 60 min IV and if this failed, electrical cardioversion. Of note, procainamide was held if patient unstable or had hx of failing procainamide in past.
Control
None
Outcomes
Primary:Conversion to sinus rhythm
Secondary: Discharge from the hospital, discharge in atrial fibrillation
Design
Retrospective, consecutive cohort study
Excluded
Patients with permanent AF, symptoms > 48 hours or an unknown duration, patients with another primary diagnosis necessitating admission.
Primary Results
Key Results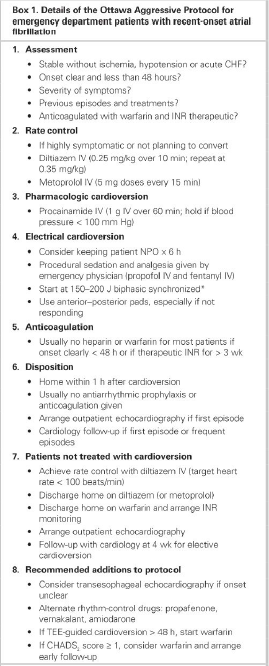
- Procainamide conversion rate: 58.3%
- Electrical cardioversion (n = 243): 91.7% success
Additional Results
- 660 patients recruited
- 95.2% with atrial fibrillation, 4.9% with atrial flutter
- Discharged home: 96.8%
- Discharged in Sinus Rhythm: 93.3%
- Relapse Rate (at 7 days): 8.6% (patients back in AF)
Adverse event rate: 7.6% (no cases of torsades, thromboembolic event or death)
Median LOS
- Converted with procainamide: 3.9 hours
- Converted with electrical cardioverion: 6.5 hours
Strengths
- Consecutive patient recruitment
- Outcomes assessed were objective thus reducing bias
Limitations
- Non-randomized
- Non-blinded
- No comparison to alternate/standard treatment
- Patients were only followed for 7 days after the intervention
Author's Conclusions
“The Ottawa Aggressive Protocol is effective, safe and rapid and has the potential to significantly reduce hospital admissions and expedite ED care.”
Our Conclusions
Although this article is 5 years old, the issue of rhythm versus rate control continues to rage on. Based on this retrospective cohort study, use of the Ottawa Aggressive Protocol appears to be safe and effective. The authors’ conclusions regarding hospital admissions and expedited ED care are not supported by this study as there is no comparison group.
Potential Impact To Current Practice
Implementation of the Ottawa Aggressive Protocol would be a reasonable approach for management of recent-onset AF. The study does not compare this protocol to standard care so we can’t comment on whether this protocol would reduce ED LOS, hospital admission or other endpoints in comparison to standard care.
Bottom Line
The Ottawa Aggressive Protocol appears to be highly effective in converting patients with recent onset atrial fibrillation or flutter back to sinus rhythm. In this cohort of 660 patients, there were no thromboembolic events and the relapse rate was 8.6% at 7 days.
Read More
Stiell IG, Birnie D. Managing recent-onset atrial fibrillation in the emergency department. Ann Emerg Med 2011; 57(1): 31-2. PMID: 21183083
Decker WW, Stead LG. Selecting rate control for recent-onset atrial fibrillation. Ann Emerg Med 2011; 57(1): 32-3. PMID: 21183084
Nuotio I et al. Time to cardioversion for acute atrial fibrillation and thromboembolic complications. JAMA 2014; 312(6): 647-9. PMID: 25117135

This is phenomenal! It’s been part of our practice at our shop for some time now, but it’s not to see it organized and explained so clearly. Thank you for posting this!