Background
CT use in the evaluation of trauma patients has risen dramatically in recent years. “Pan-scan” (CT scan from head through pelvis) is used routinely in many trauma centers in spite of the American College of Surgeons inclusion of avoidance of routine whole body CT in trauma in it’s Choosing Wisely recommendations. Although prior studies have demonstrated increased identification of traumatic pathology with “pan-scanning” there has not been a concurrent demonstration of decreased morbidity or mortality. Additionally, routine “pan-scanning” carries with it an increased radiation exposure, increased risk of cancer induction and cost. Safe reduction of CT use in trauma (decreased use without an increased miss rate of clinically significant pathology) is an area of active research.
Clinical Question
Can a decision instrument safely reduce CT imaging of the chest in adult patients with blunt trauma?
Population
All patients > 14 years of age presenting to the ED for blunt trauma within 6 hours of presentation and having chest imaging (CXR or CT Chest) ordered.
Outcomes
Chest CT-Major: Major injuries (see table 1).
Chest CT-All: All injuries (see table 1)
Design
Multicenter (8 US urban level 1 trauma hospitals), prospective observational study for both derivation and validation of a decision instrument.
Excluded
Patients < 15 years of age, no chest imaging ordered, penetrating mechanism of injury.
Primary Results
-
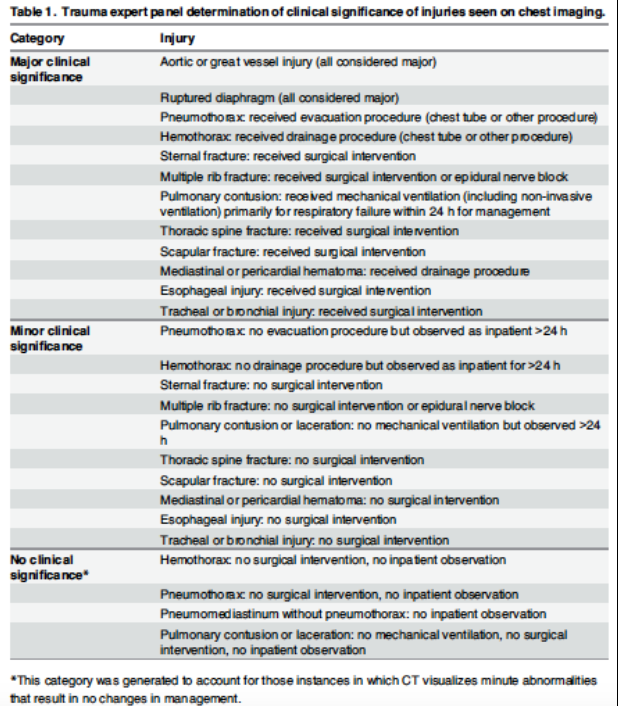
Table 1: Trauma expert panel determination of clinical significance of injuries seen on chest imaging
11,477 patients enrolled (Derivation Phase n = 6002, Validation Phase n = 5475)
- Validation phase
- 2628/5475 (48%) patients had both CXR and Chest CT
- Major Injury: 120/2628 (4.6%)
- Major or Minor Injury 706/2628 (26.9%)
- Median injury severity score (ISS) = 5
- Mechanism: MVC (35.6%), Falls (27.4%)
- Recursive partitioning used to derive Chest CT-Major and Chest CT-All decision instruments
- Chest CT-Major Criteria (all criteria must be negative)
- Abnormal CXR
- Distracting Injury (as defined by NEXUS C-spine Study)
- Chest Wall Tenderness
- Sternal Tenderness
- Thoracic Spine Tenderness
- Scapular Tenderness
- Chest CT-All Criteria
- CT-Major Criteria PLUS
- Rapid Deceleration Mechanism
Critical Findings (See Table 5 of Article)
- Chest CT-Major Decision Instrument
- Major Injury
- (-) LR: 0.03
- (+) LR: 1.5
- Major + Minor Injury
- (-) LR: 0.24
- (+) LR: 1.5
- Chest CT-All Decision Instrument
- Major Injury
- (-) LR: 0.04
- (+) LR: 1.3
- Major + Minor Injury
- (-) LR: 0.18
- (+) LR: 1.3
- Major Injury
- Major Injury
Strengths
- Multicenter and prospective
- Large n for both derivation and validation phases
- Robust (-) LR for major injuries with both CT-All and CT-Major instruments
Limitations
- Not all patients had chest CT ordered. Occult injuries may have been missed which would effect the sensitivity of the Chest CT-All decision instrument
- In the validation study, patients had to have both CXR and Chest CT to be included. Only 50% of the patients enrolled for the validation study had both imaging modalities.
- Low specificity for both CT-Major and CT-All criteria. This decision instrument should be used as a “one-direction” decision tool: a negative instrument results in a post-test probability for injury low enough to obviate the need for a chest CT in most cases but a positive criteria does NOT mandate a chest CT as the (+) LR is low.
Author's Conclusions
“We prospectively derived and validated two DIs (Chest CT-All and Chest CT-Major) that identify blunt trauma patients with clinically significant thoracic injuries with high sensitivity, allowing for a safe reduction of approximately 25%–37% of unnecessary chest CTs. Trauma evaluation protocols that incorporate these DIs may decrease unnecessary costs and radiation exposure in the disproportionately young trauma population.”
Our Conclusions
This multicenter, prospective observational study derived and validated two decision instruments with powerful negative likelihood ratios resulting from their robust sensitivities. In patients at risk for thoracic injuries after blunt trauma, negative Chest CT-Major criteria rules out the presence of clinically important injuries in the majority of patients.
Potential Impact To Current Practice
As the authors mention, proper application of these instruments can lower Chest CT imaging rates by 25-37% without resulting in a significant rise in missed clinically important injuries.
Bottom Line
The NEXUS Chest CT-Major and Chest CT-All decision instruments have the potential to decrease Chest CT imaging if carefully applied to blunt trauma patients (those in whom you would consider doing a Chest CT). It should not be applied to all trauma patients.
Read More
EM Lit of Note: NEXUS Chest (Again)
