Background
It has been recognized since the 1940s that the presence of a Left Bundle Branch Block (LBBB) obscures the EKG diagnosis of myocardial infarction (MI). The publication of the Sgarbossa criteria in 1996 aided in clarifying this issue.
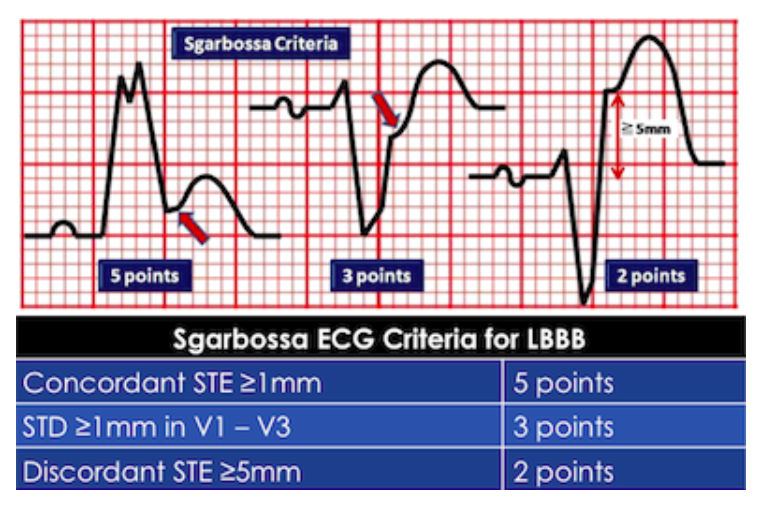
Sgarbossa Criteria (Sgarbossa 1996)
However, these criteria are not perfect. The original, weighted, Sgarbossa criteria (Sgarbossa 1996)) has an excellent specificity at 99%, but only a sensitivity of about 50%. This opens the possibility of missing a large percentage acute MIs. In 2008, Dr. Stephen Smith presented a set of modified Sgarbossa criteria, hoping to increase the sensitivity of this tool, while still maintaining a reasonable specificity (Smith 20012). This modified criteria eliminated the third criteria in the original model (Discordant STE >5mm) and instead replaced it with a new rule that’s a ratio rather than an absolute value (positive if ST elevation/S-wave amplitude <-0.25, below). The point system of the original Sgarbossa criteria was also eliminated, meaning that any one of the three modified Sgarbossa criteria is enough for a positive result.
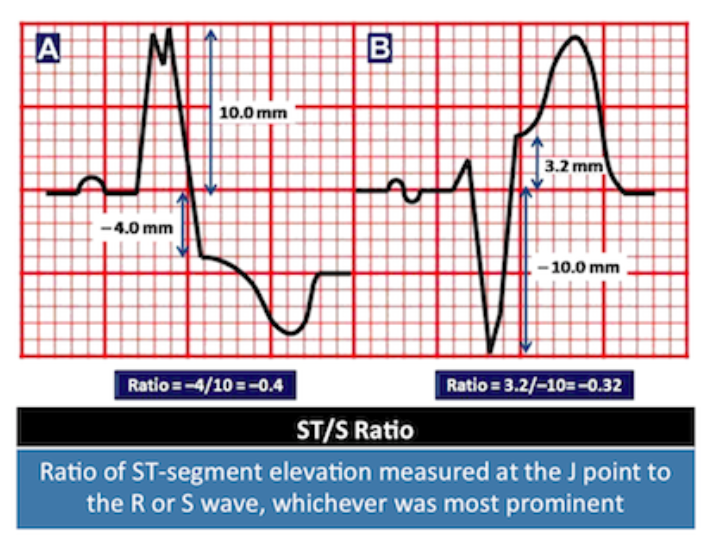
Modified Sgarbossa Criteria (Smith 2012)
Clinical Question
Can the Modified Sgarbossa Criteria be externally validated to maintain the good sensitivity and specificity demonstrated in the original derivation study?
Population
The population was obtained by chart review but, because individuals with LBBB with positive ACO were difficult to come by, a nontraditional combined cohort/case-controlled method was used to get enough charts to enroll in the study.
First, 312 of the charts came from a single hospital’s chart review. These were charts of people who presented to Duke University Hospital with an EKG with LBBB. The authors extracted charts to only include patients with possible ACS symptoms (chest pain, shortness of breath, or an anginal equivalent symptom which was defined by the physician as a symptoms “explicitly similar to the patient’s previous heart attack symptoms).
An additional 41 charts were obtained from three different hospitals by finding patients who presented with a LBBB and underwent emergent cardiac catheterization from the ED. These charts were then analyzed to see if they met the above criteria (CP, SOB, anginal equivalent as defined above).
Outcomes
Diagnostic accuracy of modified Sgarbossa criteria (in terms of sensitivity and specificity) vs the original Sgarbossa criteria for identification of acute coronary occlusion (ACO) in patients with LBBB
Design
Multicenter retrospective mixed cohort and case controlled study
Excluded
Hyperkalemia (>5.5 mEq/L), severe HTN (diastolic BP >120 mmHg), extreme tachycardia (HR > 130 bpm), pulmonary edema with respiratory distress requiring mechanical ventilation and cardiac arrest without prearrest EKG available.
Primary Results
- 45 patients were included who had LBBB and ACO
- 249 patients with LBBB and ACO were used as controls
- 312 charts were obtained from the cohort search, 54 were excluded.
Of the remaining 258, 9 had ACO and were used as cases whereas 249 were used as controls.
Critical Results
- Modified Sgarbossa Criteria vs Orignal Weighted Sgarbossa Criteria:
- Sensitivity: 80% vs 49 %
- Specificity: 99% vs 100%
- Modified Sgarbossa Criteria vs Unweighted Sgarbossa Criteria:
- Sensitivity: 80% vs 56%
- Specificity: 99% vs 94%
Strengths
- First validation of modified Sgarbossa criteria
- Multicenter nature increases external validity and applicability of results
- Publication in cardiology journal increases visibility and knowledge about the modified criteria to our specialists
Limitations
- Retrospective study meaning some eligible patients may have been missed
- Case control and cohort studies inherently have low internal validity due to selection bias
- The modified Sgarbossa criteria have not been tested in a large group of physicians so it is unclear whether it is feasible for all physicians to do the necessary calculations and if inter-rater agreement will be high
- Decision to perform cardiac catheterization is not based entirely on modified Sgarbossa criteria. This may not be reflected in this data, thus there may have been some “misses” that effect the test characteristics
- One of the three sites was Minneapolis Heart Institute, the same site as the original derivation study, so not truly and external validation study
Other Issues
-
Patients were determined to be positive for ACO if they: 1) documented ACO on cath report or 2) presumed ACO based on significant cardiac outcome (defined as A) very elevated troponin of over 10 B) new regional wall motion abnormality on ECHO or C) death before cath could be performed.
Author's Conclusions
“The modified Sgarbossa criteria were superior to the original criteria for identifying ACO in LBBB.”
Our Conclusions
We agree with the author’s conclusions but would like to see further prospective validation studies. For now, however, the modified criteria offer a simple, cheap (i.e. free) method for identifying more patients with potential ACO in the presence of a LBBB. It is highly unlikely, despite this study’s flaws, that the modified criteria decrease sensitivity since they retain the first two pieces of the original Sgarbossa Criteria. For this reason, we recommend adoption of this criteria now.
Potential Impact To Current Practice
The modified Sgarbossa criteria has the potential to increase our ability to diagnose ACO in the presence of a LBBB
Bottom Line
Use the modified Sgarbossa criteria in patients who present with LBBB on EKG and any ACS-like symptoms to determine whether the patient has a STEMI. Notably, Dr. Elena Sgarbossa of Sgarbossa criteria fame, is on record stating she supports this modified criteria (Cai 2013)
Tip: lots of talk about waiting until EKG machines incorporate ratio into their calculations/algorithms: -0.25 ratio is not that hard however. Simply measure S wave amplitude with paper, fold that paper in half twice, and compare to ST elevation. If ST elevation is greater than your folded paper, it is positive!
Read More
LITFL: Sgarbossa Criteria
REBEL EM: Modified Sgarbossa Criteria: Ready for Primetime?
Dr. Smith’s ECG Blog: Validation of Smith Modified Sgarbossa Criteria Published in American Heart Journal
References
Sgarbossa E et al. Electrocardiographic Diagnosis of Evolving Acute Myocardial Infarction in the Presence of Left Bundle-Branch Block. NEJM 1996; 334: 481-487 PMID: 8559200
Smith S et al. Diagnosis of ST-Elevation Myocardial Infarction in the Presence of Left Bundle Branch Block With the ST-Elevation to S-Wave Ratio in a Modified Sgarbossa Rule. Ann Emerg Med 2012; 60(6): 766-76. PMID: 22939607
Cai Q et al. The left bundle-branch block puzzle in the 2013 ST-elevation myocardial infarction guideline: From falsely declaring emergency to denying reperfusion in a high-risk population. Are the Sgarbossa Criteria ready for prime time? Am Heart J 2013; 166(3): 409-13. PMID: 24016487
