Background
This review was previously posted on REBEL EM here.
Predicting an anatomically and/or physiologically challenging airway is not a straightforward task by any stretch of the imagination. There are some existing difficult-airway prediction tools available (i.e. LEMON = Look externally, Evaluate 3-3-2 rule, Mallampati score, Obstruction, Neck mobility), but many of them were derived in an elective surgery setting and may not be as applicable to emergency airway management. Additionally, these prediction models only focus on anatomical challenges and ignore physiologic ones. Several components of the LEMON approach require an awake, cooperative patient. The authors of this paper derived a tool, called the HEAVAN criteria (Hypoxemia, Extremes of size, Anatomic abnormalities, Vomit/blood/fluid, Exsanguination, Neck mobility issues) to address this clinical need.
Clinical Question
Can the HEAVEN criteria accurately predict difficult airways in emergency airway management?
Population
All patients who had RSI performed by air medical providers in the US between December 2014 and November 2015
Outcomes
Intubation success
First-attempt success
First attempt success without desaturation
Design
Retrospective chart review
Excluded
None
Primary Results
- Approximately 2400 patients undergoing air medical RSI included
- Overall First attempt Intubation Success Rate = 92%
- Overall Intubation Success Rate = 97%
- 1363 (56.3%) of patients had at least one HEAVEN criteria identified
- Etomidate (75%) and Succinylcholine (80%) were the RSI medications of choice for most intubations
- The Specific Sensitivity, Specificity, PPV, and NPV of the HEAVEN criteria for first attempt success without desaturation are listed below:
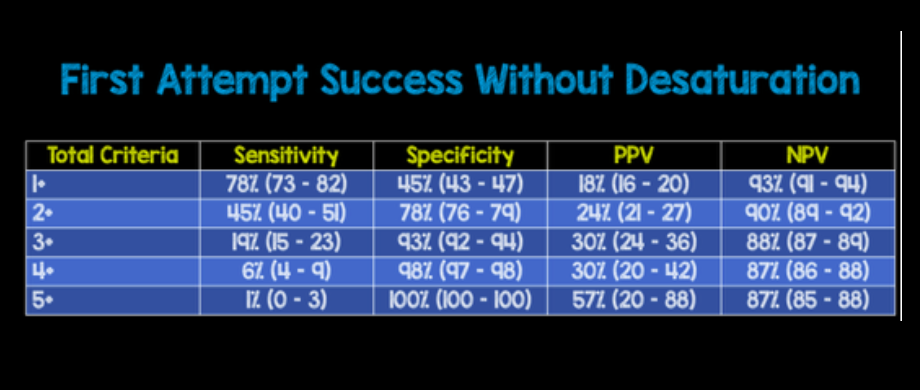
- Sensitivity and specificity evaluate a clinical test while predictive values are useful when considering the value of the test to a clinician. In this case sensitivity helps rule out a difficult airway while specificity helps rule in a difficult airway. Therefore as the number of criteria increase, so does the specificity or probability of a difficult airway. The predictive values however are not that great. Even at 5+ criteria our PPV is only 57%, meaning this criteria will fail at identifying a difficult airway in almost 1 in 2 patients (Not that useful)
Critical Results
- First attempt success lower with each additional HEAVEN criteria with an inverse relationship observed between HEAVEN criteria and intubation success
- First attempt success without desaturation is lower with each additional HEAVEN criteria with an inverse relationship observed between HEAVEN criteria and intubation success
- Vomit/blood/fluid (38%) and Neck mobility (25%) were the two most common HEAVEN criteria present
Strengths
- Large cohort of patients
- All medical providers with training in airway management (i.e. Helicopter Advanced Resuscitation Training (HeART) Program)
- Use of Apneic oxygenation and graduated escalation of preoxgenation from NRB to BVM as needed by patients
- Confirmation of ETT placement was with waveform capnography
Limitations
- Retrospective analysis of pre-hospital population
- Many of the variables evaluated at time of laryngoscopy instead of prior to attempted intubation making this tool limited in predicting airway difficulty
- Medical provider teams consist of flight nurse and paramedics in austere environments. This may limit generalizability to physicians in emergency departments
- Providers only used CMAC laryngoscope, but no other types of blades available
- After patient disposition a complete electronic medical record requiring up to 245 data elements was filled out for each patient. This retrospective nature of data collection is based on recollection and may be flawed (i.e. self – reported recollection of desaturation numbers)
- Majority of patients were trauma patients (63%) which limits generalizability to other patient groups
- Only a small group of patients had a high number of HEAVEN criteria present. This limits the ability to make sub group comparisons at higher numbers of criteria
- HEAVEN score was not compared to standard practice, so its unclear if this score would perform better or worse than clinician gestalt
Author's Conclusions
“The HEAVEN criteria seem to be a useful tool to predict difficult airways in emergency RSI.”
Our Conclusions
The HEAVEN criteria appeared to perform well in this study. However, limitations due to study design as well as absence of comparison to standard clinical assessment limits use.
Bottom Line
At this time the HEAVEN criteria cannot be recommended as an assessment of difficult airways prior to intubation in the emergency department, as the data is retrospective, in the pre-hospital setting, and the impact on airway management success has not been determined.
