Background
Atrial fibrillation (AF) is a commonly encountered dysrhythmia in the Emergency Department (ED). Atrial flutter is less common but its management is very similar to that of AF. In patients with chronic AF or unknown time of onset and a rapid ventricular response (RVR), rate control and consideration and initiation of anticoagulation therapy are the standard ED approach. Both beta-blockers and calcium channel blockers are commonly used for rate control in the ED but it is unclear whether one of these agents is superior to the other as there is scant high-quality data on the topic (Demircan 2005).
Clinical Question
Is diltiazem or metroprolol the more effective agent for rate control in AF with RVR in the ED?
Population
Adult patients > 18 years presenting with atrial fibrillation or atrial flutter.
Intervention
Diltiazem 0.25 mg/kg (max dose of 30 mg) or metoprolol 0.15 mg/kg (max dose of 10 mg) IV.
Outcomes
Primary Outcome: Heart Rate < 100 beats per minute (bpm) within 30 minutes of drug administration. Secondary Outcomes: SBP, DBP and Heart Rate at 0, 5, 10, 15, 20, 25 and 30 minutes
Design
Prospective, randomized, non-inferiority, double-blind study.
Excluded
Atrial rate < 120 bpm or > 220 bpm, SBP < 90 mm Hg, 2nd or 3rd degree AV block, Temperature > 38oC, acute STEMI, Known NYHA Class IV heart failure, chronic COPD, prehospital administration of any AV nodal blocking agent, history of allergic reaction to diltiazem or metoprolol, history of sick sinus or pre-excitation syndrome, history of anemia, pregnancy, breastfeeding or cocaine/methamphetamine use within 24 hours.
Primary Results
Critical Findings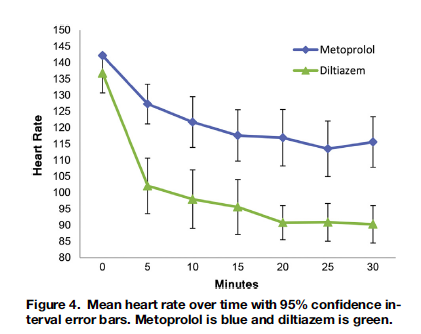
- Primary Outcome (HR < 100 bpm at 30 min)
- Diltiazem group 95.8% vs. Metoprolol group 46.4% (p < 0.0001)
- Diltiazem had more rapid rate control than metoprolol at every time interval measured
- No difference in bradycardia events or hypotension events between groups
Primary Results
- 54 patients met inclusion criteria (diltiazem n = 25, metoprolol n = 29)
- 52 patients included in analysis (1 excluded post-randomization from each intervention group)
Strengths
- Although small, this is the largest RDCT comparing diltiazem versus metoprolol head to head
- Randomization and blinding were well done
Limitations
- Convenience sample of patients
- Group initially calculated an n = 200 patients to achieve 80% power to detect noninferiority. However, they only collected 52 patients due to interim analysis showing a large benefit. It is possible that the results would have regressed towards the mean if complete enrollment was performed.
Other Issues
- About 20% of patients in both groups received adenosine at some point
Author's Conclusions
“Diltiazem was more effective in achieving rate control in ED patients with AFF and did so with no increased incidence of adverse effects.”
Our Conclusions
Diltiazem is non-inferior to metoprolol for rapid rate control in patients with AF and RVR. Larger, multicenter RDCTs are needed.
Potential Impact To Current Practice
This study helps to defend what is the most common practice in the ED for patients with AF and RVR who require rate control.
Bottom Line
The best available evidence demonstrates that diltiazem achieves rate control faster than metoprolol in patients with AF and RVR. Diltiazem should be considered the first line agent.
Read More
ALiEM: Atrial Fibrillation Rate Control in the ED: Calcium Channel Blockers or Beta Blockers.
ALiEM: Beta Blockers Vs. Calcium Channel Blockers for Atrial Fibrillation Rate Control: Thinking Beyond the ED.
References
Demircan C et al. Comparison of the effectiveness of intravenous diltiazem and metoprolol in the management of rapid ventricular rate in atrial fibrillation. Emerg Med J 2005;22:411–4. PMID: 15911947
