Background
Warfarin and clopidogrel are two commonly prescribed anticoagulant medications, and based on previous studies, patients taking either of these medications who suffer blunt head trauma are at an increased risk for traumatic intracranial hemorrhage (ICH). Additionally, there is concern that patients on these agents can have delayed traumatic ICH (traumatic ICH occurring within 2 weeks after an initially normal CT scan result in the absence of recurrent head trauma). Guidelines at many hospitals recommend routine head CT imaging and admission for neurologic observation in patients who suffer head trauma while taking warfarin. Evidence to inform guidelines for management of minor head trauma patients on clopidogrel is lacking. Despite the presence of hospital protocols for routine observation of both patient groups, there is little literature looking at the incidence of immediate and delayed traumatic ICH in patients taking warfarin or clopidogrel.
Clinical Question
What is the incidence of immediate and delayed traumatic intracranial hemorrhage in patients with blunt head trauma who are receiving clopidogrel or warfarin?
Population
Adults 18 years or older with blunt head trauma who are taking either warfarin or clopidogrel (within the last 7 days)
Outcomes
Immediate and delayed (at 14 days) traumatic ICH
Design
Prospective observational study
Excluded
Patients with known injuries transferred from other facilities, patients taking both warfarin and clopidogrel
Primary Results
- 1064 adult head trauma patients included in the study
- 768 patients on warfarin
- 296 patients on clopidogrel
Critical Results
- Immediate traumatic intracranial hemorrhage: 70/1000 (7.0%; 95% CI 5.5% to 8.8%)
- Patients on clopidogrel: 12.1% (33/276)
- Patients on warfarin: 5.1% (37/724)
- RR = 2.31 (95% CI 1.48-3.63)
- Delayed traumatic ICH: 0.4% (4/930)
- Patients on clopidogrel: 0.0% (0/243)
- Patients on warfarin: 0.6% (4/687)
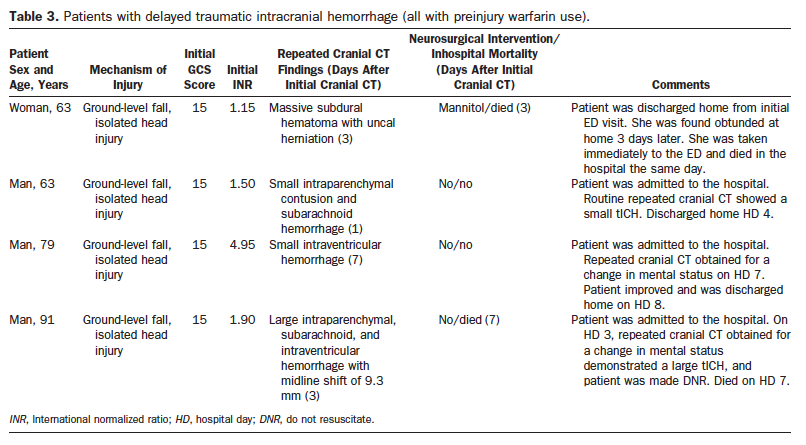
- 2/4 patients with delayed ICH died (Care withdrawn in 1 and the other found obtunded at home and died in hospital)
Strengths
- Study enrolled a large number of patients
- Multicenter study drawing patients from both trauma centers and community hospitals thus increasing the external validity.
- Included patients with any degree of head trauma
- Excellent follow up (99.5%)
- The authors discuss the details of all 4 patients with delayed ICH (table 3)
Limitations
- Selection bias – likely patients with more concerning physical exam findings were ordered for CT scans, potentially missing patients who suffered traumatic ICH
- Follow up was performed by standardized phone interview at 14 days not in person
Author's Conclusions
“ED patients with blunt head trauma and preinjury clopidogrel use have a significantly higher prevalence of immediate traumatic intracranial hemorrhage compared with those with preinjury warfarin use. Routine cranial CT imaging is generally indicated in patients with blunt head trauma who are receiving clopidogrel or warfarin, regardless of the clinical findings. The cumulative incidence of delayed traumatic intracranial hemorrhage is very low for both groups, suggesting that in patients with a normal cranial CT scan result, anticoagulation reversal is unnecessary and discharging them home from the ED may be reasonable.”
Our Conclusions
This study demonstrates that patients on either clopidogrel or warfarin are at significant risk of ICH after head injury. A NCHCT should be considered in all patients taking either warfarin or clopidogrel with any degree of head injury. The rate of delayed ICH, however, is extremely low. Based on the numbers in this paper, admitting all patients for observation would lead to the diagnosis of 1 delayed ICH for every 232 admissions.
Potential Impact To Current Practice
This study recognizes the importance of obtaining head CT scans in patients on warfarin or clopidogrel. The results of the study also suggest that patients on warfarin/clopidogrel with an initial negative head CT scan are unlikely to need admission for repeat imaging, but need reliable follow-up.
Bottom Line
While immediate ICH is common in patients on warfarin or clopidogrel who suffer any head trauma, delayed ICH is rare. Routine observation and repeat imaging in patients with an initial negative NCHCT has an extremely low yield.
Read More
Li J. Validation of the Dime. Ann Emerg Med 2012; 59 (6): 469 – 70. PMID: 22626016
Alrajhi KN. Intracranial bleeds after minor and minimal head injury in patients on warfarin. J Emerg Med 2015; 48(2): 137-42. PMID: 25440860
REBEL EM: Minor head trauma in anticoagulated patients: admit for observation or discharge?
3 of the 4 initially had sibtherapeutic INR! And the one that I classically think about (super therapeutic INR) seems like the delayed bleed was pretty minor.