Background
Triage and prioritizing patient care is an important skill that Emergency Medicine physicians must develop to become efficient and effective providers. Previous studies have demonstrated statistically significant delays in door to provider time due to race and volume in the ED (Okunseri 2013, Sonnenfeld 2012). No previous study has investigated variances in door to provider time based on chief complaint. If such a relationship exists it would be useful to compare perceived and idealized prioritization to actual resident behavior. Additionally, inclination of residents to avoid or delay taking on patients with certain complaints may highlight educational needs.
Clinical Question
Is there a relationship between door to provider time, or in this study, “patient pick-up time” and chief complaint?
Population
All adult patients presenting to a single, academic Emergency Department (ED) from August 1st 2012 – July 31st 2013.
Outcomes
Patient Pickup Time: defined as the difference between the time the patient was seated in the ER and the time a resident assigned themselves to the patient
Design
Single-center retrospective observational study using a parametric proportional hazard model w/ Weibull distribution for analysis
Excluded
Any records where some of the required fields were incomplete
Patients who were primarily seen by an attending
Trauma patients, given that they are typically seen immediately and prior to self assignment
Visits where pick-up time exceeded 60 minutes were determined to be outliers secondary to tracking board errors or miscommunications in assignment
Primary Results
- 45,312 total patient visits
- 14,930 (32.9%) were excluded leaving 30,382 (67.1%) patient visits for analysis
Critical Results
- Median pickup time was 6 minute (interquartile range 2-15 minutes)
- Shortest pickup times: ankle injury, allergic reaction, wrist injury
- Longest pickup times: vaginal bleeding, numbness/tingling and abdominal pain
- The 10 fastest and 10 slowest chief complaint pickup times are included below:
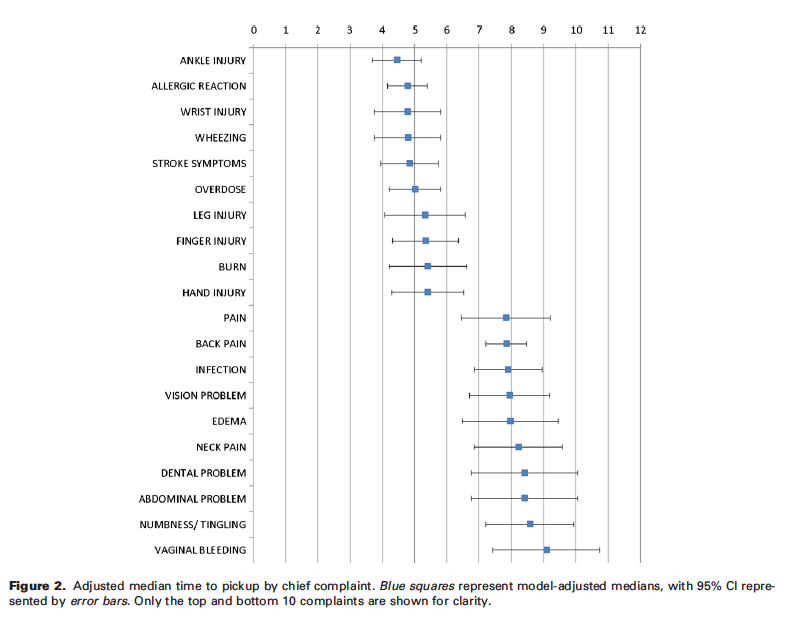
(Patterson 2016)
Strengths
- Only study to date looking at effect of chief compliant on resident “pick-up time”
- Adjusted for known and intuitive co-variables
Limitations
- Single center retrospective study only representing the patients and biases of a single ED and residency program
- Authors were not able to exclude or adjust for periods of time in the ER when there was only a single resident present, possibly skewing minimizing differences or underlying biases related to specific chief complaints
Author's Conclusions
“A consistent variation in resident pickup time exists for common chief complaints. We suspect that this reflects residents preferentially choosing patients with simpler workups and less perceived diagnostic ambiguity. This work introduces pickup time as a metric that may be useful in the future to uncover and address potential physician bias. Further work is necessary to establish whether practice patterns in this study are carried beyond residency and persist among attendings in the community and how these patterns are shaped by the information presented via the EHR.”
Our Conclusions
This study revealed a statistically significant difference in resident pickup time among chief complaints. Residents in this study took longer to pick up patients with particular chief complaints (i.e. vaginal bleeding, back pain, numbness/tingling). Although statistically significant, it is unclear whether the relatively small differences in pick up time (3-5 minutes) have any clinical relevance or whether these differences persist after training. This may reflect a preference for cases with simpler workups, less diagnostic ambiguity or avoidance of possible uncomfortable patient interactions.
Potential Impact To Current Practice
Residents should be mindful of their potential biases, specifically towards chief complaints that may be personally difficulty or have a nebulous workup. Awareness of these biases can help prevent the development of gaps in fund of knowledge and remedy existing gaps.
Bottom Line
Current evidence, although limited, suggests that residents preferentially choose patients with simpler workups with less perceived diagnostic ambiguity.
Read More
References
Okunseri C et al. Racial and ethnic variations in waiting times for emergency department visits related to nontraumatic dental conditions in the United States. J Am Dent Assoc 2013; 144: 828–36. 23813265
Sonnenfeld N et al. Emergency department volume and racial and ethnic differences in waiting times in the United States. Med Care 2012; 50: 335–41. 22270097