The Case
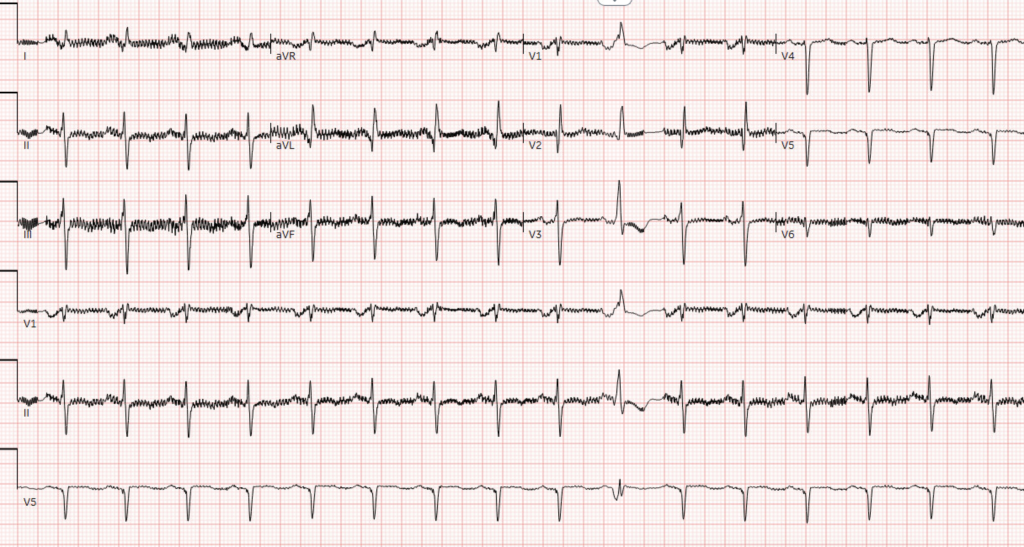
A 40 year old male with a history of obstructive coronary artery disease (remote percutaneous intervention), heart failure with severely reduced ejection fraction (10%), left ventricular assist device (LVAD) placed 2022, presents to the emergency department with acute onset of chest pressure and light-headedness. The patient denies any LVAD alarms prior to arrival. The following ECG is obtained:
EKG

Show Details
EKG Characteristics
-
Rate
231
-
Rhythm
Wide QRS Tachycardia
-
Intervals
QRS 142 ms, QTc 419 ms
Diagnosis
Ventricular Tachycardia
Wide complex tachycardia should be presumed ventricular tachycardia until proven otherwise, especially if no prior history of widened QRS. Comparison to prior ECG’s may reveal a prior intra-ventricular conduction delay (bundle branch block) to support a supra-ventricular tachycardia with aberrancy.
Other features that support ventricular tachycardia include:
- AV dissociation (P waves marching through QRS complexes)
- Capture and/or fusion beats
- Extreme axis deviation
- Concordance in pre-cordial leads
Questions
-
What is the differential diagnosis for this patient?
Ventricular tachycardia, supraventricular tachycardia with aberrancy.
Discussion
Ventricular tachycardia (VT) is common in the LVAD population (> 50% of patients). Underlying risk factors for VT include:
- Underlying cardiomyopathy
- Right-ventricular (RV) failure
- Mechanical compression of the ventricle by the inflow cannula
- Less commonly, VT can be due to myocardial ischemia/infarction from native coronary artery disease
Due to the degree of physiologic support afforded by the LVAD (continuous flow physiology), otherwise fatal arrhythmias are often well-tolerated, and may present with vague symptoms such as fatigue, nausea, light-headedness, or chest pressure.
As VT or VF may be tolerated for a short period in LVAD patients, clinicians often have time to try medical interventions prior to resorting to electrical cardioversion. In the hemodynamically stable LVAD patient:
- Evaluate for mechanical etiology of VT.
- Point-of-care ultrasound may demonstrate an overly decompressed LV with collapse and septal shift
- Decreasing LVAD speed or a fluid bolus may allow for increased ventricular filling and resolve the arrhythmia
- Anti-arrhythmic agents such as amiodarone and lidocaine should be considered in the absence of a mechanical cause of arrhythmia.
- Cardioversion and defibrillation are not contraindicated and can be performed without disconnection of the LVAD device.
- Use an anterior-posterior pad placement
- Avoid placing pads over the LVAD pump
- Consider sedation if the patient is concious
- Patients with recurrent VT from increased sympathetic tone may benefit from high-dose beta-blockers.
The patient was treated with an amiodarone bolus which terminated the rhythm. He was subsequently admitted to advanced cardiology for further diagnostics and cardiac monitoring.
Pearls
- Assume ventricular tachycardia until proven otherwise in patients presenting with wide QRS tachycardia.
- ECG's obtained on LVAD patients may contain considerable artifact, compare to prior ECG's when possible.
- Typically unstable arrhythmias may be well-tolerated in patients with LVADs due to the continuous flow physiology of the mechanical pump. In hemodynamically stable patients, evaluate for mechanical etiology of arrhythmias and consider appropriate anti-arrhythmic medications.
- Electrical cardioversion is safe in LVAD patients. Avoid placing pads directly over the LVAD pump. Pursue an anterior-posterior approach and use sedation on the concious patient.
Sources
Givertz MM, DeFilippis EM, Colvin M, et al. HFSA/SAEM/ISHLT clinical expert consensus document on the emergency management of patients with ventricular assist devices. J Heart Lung Transplant. 2019;38(7):677–698. doi:10.1016/j.healun.2019.05.004
