The Case
A 41-year-old male presents to the ED with constant palpitations for one day. The patient's medical history is notable for a congenital bicuspid aortic valve, four months post aortic valve replacement with a post-surgical ejection fraction of 30%. The following ECG is obtained:
EKG

Show Details
EKG Characteristics
-
Rate
Tachycardic (142)
-
Rhythm
Regular, Non-sinus
-
Intervals
Wide complex QRS (146 ms)
-
Axis
Left axis deviation
-
ST Segments
Non-specific
-
Additional Features
Right bundle branch block morphology
Diagnosis
Idiopathic Fascicular Ventricular Tachycardia
Questions
-
What is the differential diagnosis for this ECG?
The differential diagnosis for this patient includes Ventricular Tachycardia (VT) and Supraventricular Tachycardia (SVT) with aberrancy. Differentiating between the two is difficult as multiple proposed diagnostic criteria have yet to demonstrate sufficient sensitivity or specificity for a definitive diagnosis.
Discussion
Fascicular VT is a distinct subgroup of idiopathic VT. Fascicular VT is reentrant tachycardia due to an ectopic focus within the left ventricle, most commonly in the fascicles. Unlike other forms of VT, Fascicular VT may be more likely to be misidentified as SVT with aberrancy, given RBBB morphology and lack of precordial concordance.
The location of the re-entry circuit determines the morphology of Fascicular VT:
Posterior fascicular VT (most common):
- RBBB + left axis deviation; arises close to the left posterior fascicle
Anterior fascicular VT:
- RBBB + right axis deviation; arises close to the left anterior fascicle
Upper septal fascicular VT (rare):
- Usually RBBB but can be LBBB, narrow QRS with normal axis; arises from the upper septum
Treatment of fascicular VT:
Unstable: Synchronized Cardioversion
Stable:
- IV Verapamil
- Sotalol and Amiodarone
- Radio-frequency ablation
Vagal maneuvers, adenosine, lidocaine, and beta-blockers are unlikely to affect this rhythm. Adenosine may reveal capture or fusion beats to assist in diagnosis; however, this should be performed in conjunction with specialty recommendation.
Ventricular Tachycardia vs. Suprabentricular Tachycardia with Aberrancy:
Factors that may suggest Ventricular Tachycardia or Supraventricular Tachycardia include:
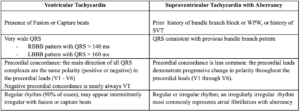
Up to 80% of all patients who present with a wide complex tachycardia will be diagnosed with ventricular tachycardia. Risk factors that increase the likelihood of VT include history of previous myocardial infarction, known coronary artery disease, and structural heart disease. Increased age is also an independent risk factor for increased likelihood of VT in wide complex tachycardia. When in doubt, treat as ventricular tachycardia.
Case Outcome:
The patients EKG performed in the ED showed a Wide Complex Tachycardia at a rate of 142 bpm. He was mentating appropriately with a blood pressure of 105/77.
This patient was given a bolus of Amiodarone and subsequently started on a drip. With the guidance of cardiology, the patient was given adenosine to assist in determining the underlying rhythm. A capture beat was noted on the rhythm strip, suggesting ventricular tachycardia as the underlying rhythm. The patient did not respond to medical therapies trialed in the emergency department and ultimately underwent radio-frequency ablation with the return of normal sinus rhythm. His condition remained stable, and he was discharged home the following day.
Pearls
- Consider ventricular tachycardia in any unexplained tachycardia with a widened QRS (especially in patients history of narrow QRS on prior ECG or no previous ECG for comparison).
- Fascicular VT is a distinct subgroup of ventricular tachycardia; it may commonly be mistaken for SVT with aberrancy due to “innocuous” RBBB appearance.
- Fascicular VT can occur in young, healthy patients with and without structural heart disease.
- Fascicular VT often does not respond to typical VT (or SVT) therapies; however, it is likely to be responsive to Verapamil or radio-frequency ablation.
Sources
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1501077/
- https://emj.bmj.com/content/19/5/477
- https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-9/Idiopathic-fascicular-left-ventricular-tachycardia
- https://accessemergencymedicine.mhmedical.com/content.aspx?bookid=2969§ionid=250463206#:~:text=When%20a%20person%20with%20a,a%20ventricular%20tachycardia%20(VT).
- Brady WJ, Skiles J. Wide QRS complex tachycardia: ECG Differential diagnosis. AM J Emerg Med. 1999;17(4):376-381

