Definition: Encephalopathy that occurs secondary to thiamine (vitamin B1) deficiency. While Wernicke encephalopathy is reversible with treatment, it can progress to the irreversible Korsakoff’s syndrome if left untreated.
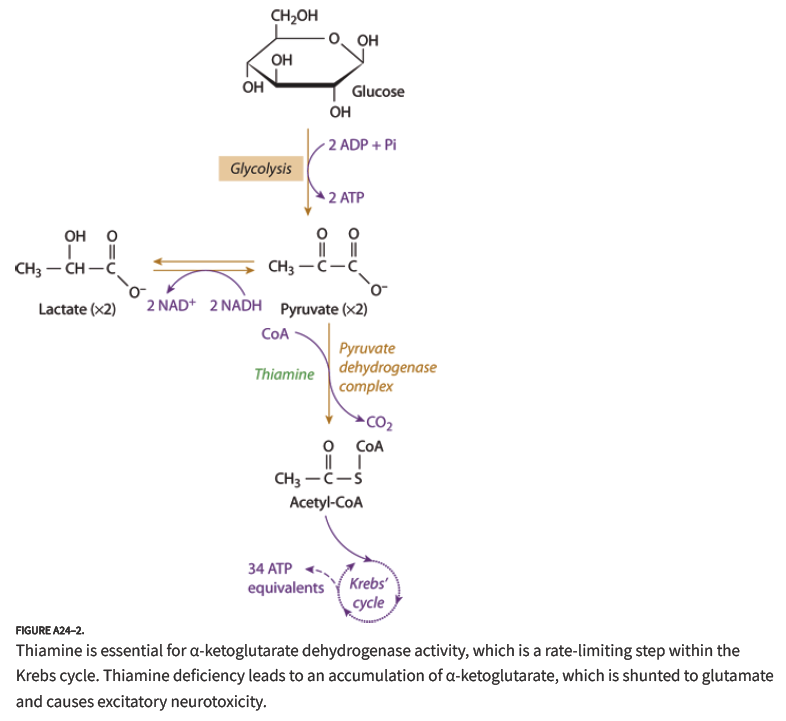
Thiamine in the Krebs Cycle (Goldfrank’s Toxicology)
Pathophysiology
- Thiamine is a cofactor for the enzyme pyruvate dehydrogenase
- This enzyme converts pyruvate to acetyl-CoA
- Acetyl-CoA enters the Krebs cycle and ATP is produced
- Without thiamine, the Krebs cycle breaks down leading to ATP depletion affecting the brain and heart
At Risk Populations
- US incidence of 0.2 – 2% (Hoffman 2015)
- Affects people with malnutrition or malabsorption
- Specific groups
- Chronic alcoholics
- Bariatric surgery patients
- AIDS patients
- Active malignancy
- Hyperemesis gravidarum
- Eating disorder patients
- Bone marrow transplant recipients
- CHF on furosemide (furosemide enhances renal elimination of thiamine)
History and Physical Examination
- Patients will have a history of malnutrition or malabsorption
- Classic Triad
- Ataxia
- Ophthalmoplegia (classically nystagmus and lateral rectus palsy)
- Altered Mental Status/Confusion
- All three features present in < 10% of patients (Donnino 2007)
- Hypotension and hypothermia may be seen
- Elevated lactate levels are common due to interruption of the Krebs cycle (Donnino 2007)
- Clinical Assessment Tool
- Dietary deficiencies
- Oculomotor abnormalities
- Cerebellar dysfunction
- Altered mental status or mild memory impairment
- > 2 of above components is diagnostic
 Management
Management
- Preventive care: Thiamine 100 mg IV/IM
- Parenteral route recommended as many of these patients have abnormal GI absorption
- IV better than IM as many patents have diminished muscle mass making absorption less predictable
- Should be provided to all groups at risk of thiamine deficiency (see above)
- Unclear how long this provides protection for. Best estimates are about 1-2 weeks (Hoffman 2015)
- Treatment of Wernicke’s Encephalopathy
- Basics
- Check glucose and supplement as needed
- Check electrolytes as concomitant electrolyte deficiencies (magnesium, potassium etc) are common
- Thiamine 500 mg IV Q8 X 3 days
- Follow with thiamine 250 mg IV Q24 X 3-5 days
- Ophthalmoplegia can improve in hours while altered mental status and ataxia are frequently more delayed in improvement if they improve at all
- Basics
Take Home Points
- Wernicke encephalopathy is characterized by ataxia, altered mental status and ophthalmoplegia but patients are unlikely to have all these components
- Suspect Wernicke encephalopathy in any patient that is at risk of malnutrition or malabsorption and has any one of the classic symptoms
- Prophylactic administration of thiamine 100 mg IV/IM to at risk patients can prevent development of the disease
- Once Wernicke encephalopathy has developed, it must be treated with high-dose, IV thiamine
Read More
ER Cast: What You Don’t Know About Wernicke’s Encephalopathy
LITFL: Thiamine Deficiency
EMRAP: Remember to Take Your Vitamins
ALiEM: Mythbusting the Banana Bag
References
Hoffman RS. Antidotes in Depth. In: Hoffman RS, Howland M, Lewin NA, Nelson LS, Goldfrank LR. eds. Goldfrank’s Toxicologic Emergencies, 10e New York, NY: McGraw-Hill; 2015. [Access Emergency Medicine]
Donnino MW et al. Myths and Misconceptions of Wernicke’s Encephalopathy: What Every Emergency Physician Should Know. Ann Emerg Med 2007; 50: 715-21. PMID: 17681641
