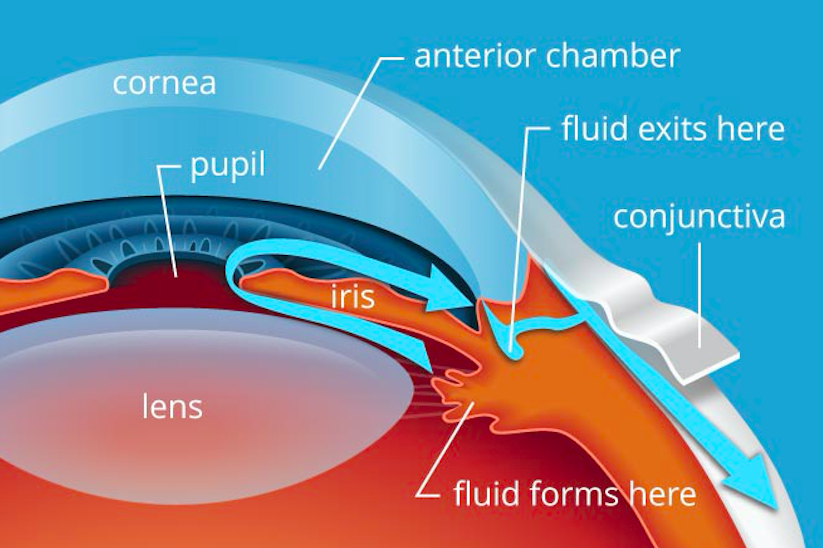
Eye Anatomy (www.allaboutvision.com)
Definition: Decrease of visual acuity due to a non-traumatic cause. Transient vision loss defined as vision loss <24 hours. Persistent vision loss defined as loss of vision >24 hours. (Bagheri 2015).
Causes: There are multitude of causes of vision loss. This post focuses on the following pathologies:
- Glaucoma
- Giant Cell Arteritis
- Vitreous Detachment
- Retinal Detachment
- Central Retinal Vein Occlusion
- Central Retinal Artery Occlusion
- Amaurosis Fugax
Glaucoma (Weinreb 2014, Schmidl 2015)
Definition: A group of diseases that have increased intraocular pressure (IOP), causing damage the optic nerve leading to decreased vision
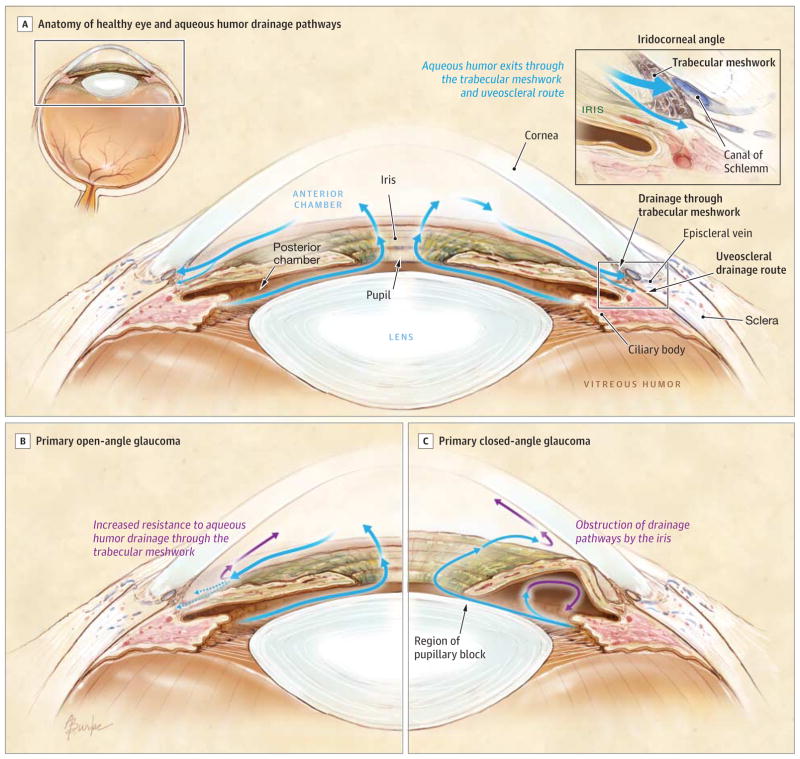
Glaucoma Anatomy (Weinreb 2014)
| Open angle | Closed angle | |
| Definitions | Increased resistance to aqueous outflow through the trabecular meshwork. | Access to the drainage pathways is obstructed |
| Pathophysiology | Increase in IOP; Exact etiology unclear, but has a normal appearing anterior chamber angle and raised intraocular pressure (IOP). Asymptomatic until late in disease after vision loss occurs. Most common type of glaucoma | Occurs with obstruction to aqueous outflow, usually from the iris. Most common cause: pupillary block. |
| Symptoms | Generally painless, asymptomatic. May have blurred vision or decreased visual acuity. | Painful vision loss, classically when going into a dark room. Other symptoms include halos around lights, nausea and vomiting. |
| Signs | IOP >21. Decreased visual acuity, Cup to disc ratio >0.6 (difficult to see due to corneal edema) | IOP >21 (often >60), conjunctival injection, corneal edema, pupil that is hazy, fixed, mid-dilated. Cup to disc ratio >0.6 (difficult to see due to corneal edema) |
Emergency Department Management
- All patients should get emergency ophthalmologic consultation
- Start with eye drops (see table below) and add systemic medications if severe or refractory symptoms/IOP
- 1st line med: Timolol (beta blocker)
- Topical meds can be given simultaneously except for pilocarpine. Pilocarpine is typically not effective until IOP is < 40 mmHg
| Drug | Class | Dose | Mechanism | Side effects |
| Timolol 0.5% | Beta blocker | 1 gtt | Reduces production of aqueous humor via decreasing cAMP concentration in the ciliary body | Can cause systemic effects, so if the patient has any contraindication to beta blocker, don’t use it. (contraindications = asthma, chronic obstructive pulmonary disorder, and patients with second and third degree heart blocks) |
| Apraclonidine 1% | Alpha agonist | 1-2 gtt | Reduces production of aqueous humor plus increases outflow via contraction of the ciliary body | CNS effects and respiratory arrest in young children; caution in patients with cerebral or coronary insufficiency, postural hypotension, and renal or hepatic failure |
| Pilocarpine 1-2% | Cholinergic | 1 gtt Q15 mins until IOP <40
Given after Timolol |
Causes iris to contract (miosis), which opens the canal more. Also can contract smooth muscle cells in the ciliary body, leading to an increase in aqueous outflow by widening the trabecular mechwork and Schlemm’s canal | Ciliary spasm leading to headaches in young patients
Ineffective at IOP >40 mmHg |
| Latanoprost | Prostaglandin | 1 gtt | Increase drainage through the uveoscleral outflow path. | Minimal systemic adverse effects; may be related to headaches |
| Acetazolamide | Carbonic anhydrase inhibitor | 500 mg IV/PO | Reduces production of aqueous humor (CA makes bicarb, which is a major component of the aqueous humor) | Topical form has minimal systemic adverse effects; oral form may be associated with paresthesia, nausea, diarrhea, loss of appetite and taste, lassitude, or renal stones.
Caution in sickle cell patients. |
| Mannitol | Hyperosmotic agent | 1-2 grams/Kg IV | Reduces production of aqueous humor. | To minimize cerebral effects, and typically reserved if topical medications and acetazolamide do not work within 1 hour (from Rosens) |
Pro Tip: Can decrease systemic absorption of topical drops by putting pressure over medial surface of eye (over lacrimal duct) while placing drops.
Giant Cell Arteritis (arteritic anterior ischemic neuropathy) (Bagheri 2015, Hayreh 2009)
Pathophysiology
- Giant cell arteritis(GCA) affects that medium-sized and large arteries.
- T-cell-dependent disease.
- Predilection to involve the posterior ciliary artery. If not treated promptly, can cause profound bilateral visual loss without expeditious systemic corticosteroid treatment
Symptoms
- Often present with systemic symptoms, including anorexia and weight loss, malaise, myalgias
- Jaw claudication (can have tongue claudication as well)
- Headache (⅔ have this as primary symptom)
- Scalp tenderness
- Abnormal temporal artery and neck pain, myalgia, malaise and anemia.
- Transient unilateral vision loss (amaurosis fugax)
- Eye itself is usually painless.
Signs
- Decreased visual acuity common, but normal visual acuity does not rule out disease.
- Funduscopic exam:
- Classic finding is a pale ‘‘chalky white” swollen optic nerve head (70% of patients) (Hyreh 1998)
- Relative APD.
Lab tests
- Erythrocyte sedimentation rate (ESR).
- Typically will see marked elevation.
- A normal ESR does not rule out GCA
- C-reactive protein (CRP): CRP is the more sensitive marker for GCA
- Get both, because a positive ESR and CRP is close to 100% specific (Hayreh 2009)
- Gold standard test: temporal artery biopsy
Emergency Department Management
- Ophthalmology/rheumatology consultation
- Prednisone: 80-100 mg Q24
- Ideally, start steroids after biopsy performed
- If high suspicion, start empiric steroids as unlikely to markedly alter biopsy results
- Duration of steroids (Hayreh 2009)
- Until the CRP and ESR go back down to normal
- Often takes 2-3 weeks.
- Followed by a steroid taper
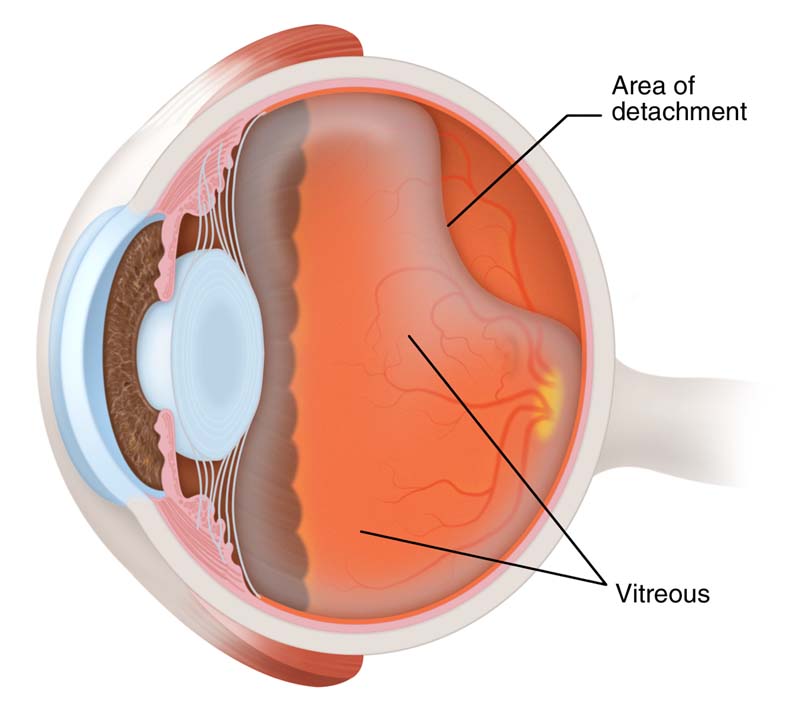
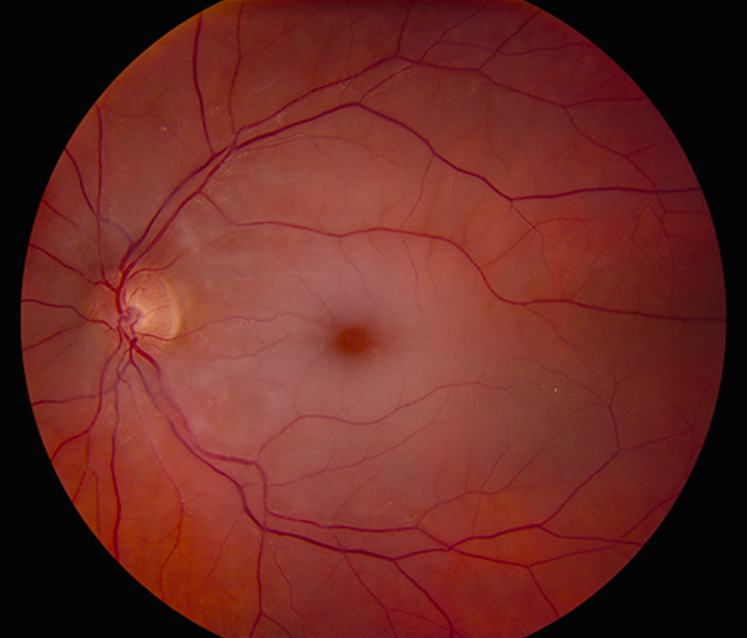
Vitreous Detachment (jaheedkhan.co.uk)
Vitreous Detachment (Guluma 2018)
Definition: Separation between the posterior vitreous cortex and the internal limiting membrane (ILM) of the retina (which is the most external portion of the retina).
Background
- Risk factors – Increasing age, myopia (nearsightedness)
- Many older individuals have essentially asymptomatic vitreous detachments.
- Often occurs as the vitreous shrinks with increasing age, pulling away from the retina.
Symptoms
- Floaters > flashers
- No change in visual fields
- May have decreased visual acuity.
Signs
- Shafer’s sign (tobacco dust)
- May see a Weiss ring when the posterior vitreous (PV) detaches from the optic disc margin
- Visualization with ultrasound.
Emergency Department Management
- Emergency ophthalmology consultation
- Emergency surgical management indicated if concomitant retinal tear, vitreous hemorrhage, or retinal detachment

Retinal Detachment (webeye.ophth.uiowa.edu:)
Retinal Detachment (Hollands 2009)
Pathophysiology
- Posterior vitreous shrinks with advancing age (aka synchysis senilis), pulling on the retina.
- Pulling can cause tears in the retina (10-15% of the time) (Hollands 2009)
- Tear allows liquefied vitreous leaks in, causing the retina to separate from the retinal pigment epithelium (33-46% of the time) (Hollands 2009)
Symptoms
- Blurry vision/decreased peripheral vision
- Flashers(photopsia)/floaters
- 14% of pts referred to ophthalmology with flashers/floaters end up having retinal tears.
- Photopsia is from vitreoretinal traction, floaters are from vitreous cells/blood in the eye.
- Symptom characteristics (Hollands 2009)
- Any flashers/floaters: (+) LR 1.2 and (–) LR 0.9.
- >10 floaters, (+) LR 8.1-36
Signs
- Pigmented cells (‘‘tobacco dust’’ aka Shafer’s sign) in the vitreous and occasionally in the anterior chamber (caused by pigmented epithelial cells that spilled into vitreous)
- Visual field loss
- Vitreous hemorrhage: (+) LR 10
- Visualization on ultrasound

Ocular US Normal (aliem.com)
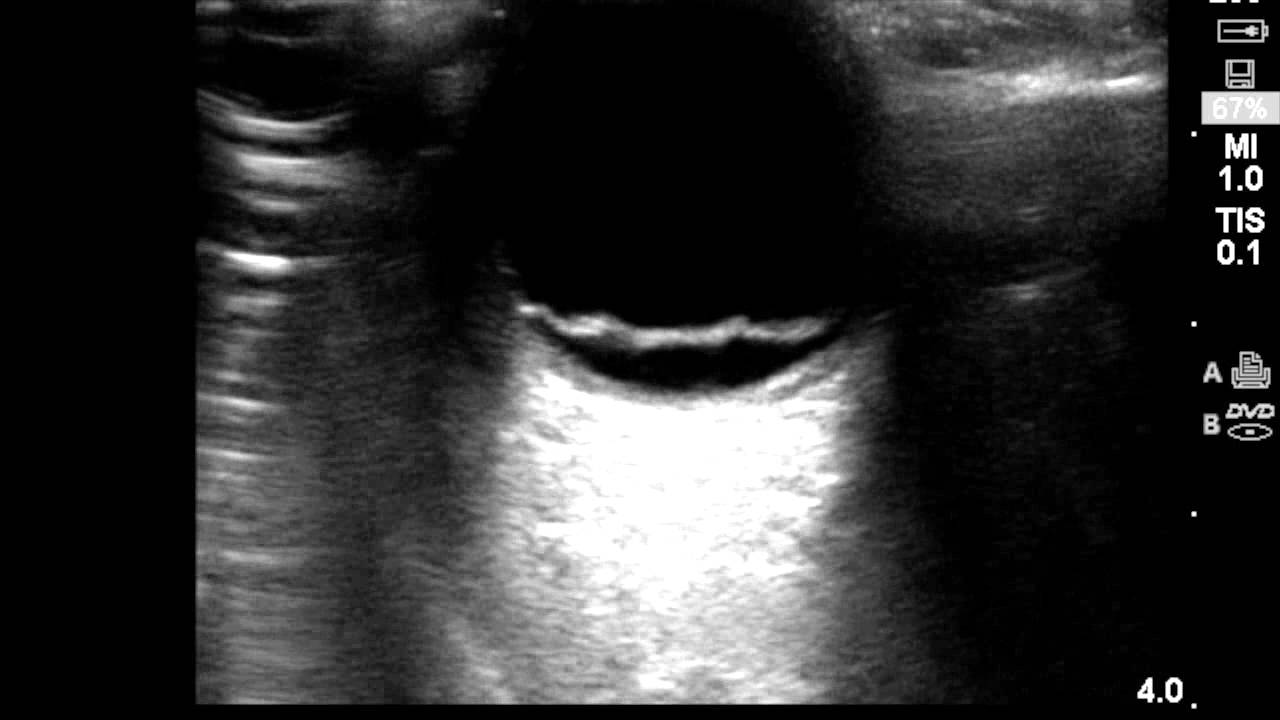
Retinal Detachment US (youtube.com)
Emergency Department Management
- Emergency ophthalmology consultation for possible surgical repair
Central Retinal Vein Occlusion (CRVO) (McAllister 2012)
Background
- Pathophysiology not fully understood; possibly due to thrombus located in the central retinal vein (CRV), in the region of the lamina cribrosa
- Second most common cause of vision loss due to retinal vascular disease (Most common cause: Diabetic retinopathy)
Symptoms
- Floaters – CRVO can cause neovascularization which causes leaky vessels leading to debris in vitreous.
- Blurry vision
- Glaucoma symptoms – due to leaky vessels.
- May be asymptomatic
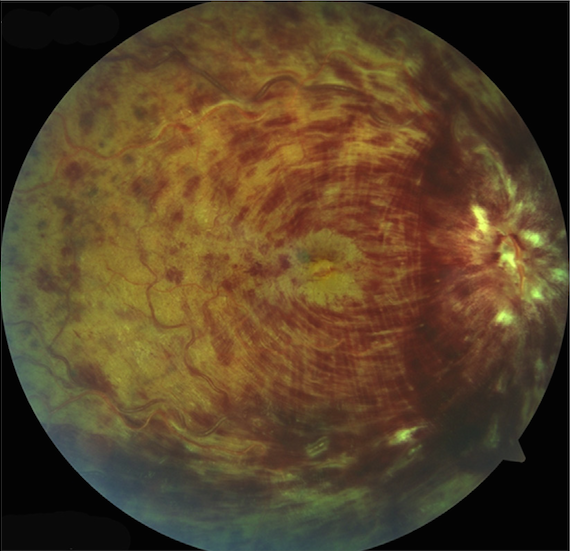
Central Retinal Vein Occlusion (Bagheri 2015)
Signs
- Visual acuity deficit – Variable degree.
- Funduscopic exam-
- Flame-shaped, dot and blot hemorrhages
- Retinal edema: May be limited to a certain section of the retina (if branch occlusion) or in all quadrants (if central vein occluded) (aka pizza pie eye)
- May have macular edema
Emergency Department Management
- Ophthomology consultation
- Treatment traditionally laser for neovascularization complications, although newer treatments are emerging.
Central Retinal Artery Occlusion (CRAO)
Background
-
- Anatomy: First branch of the internal carotid artery is the ophthalmic artery which splits into the posterior ciliary and central retinal arteries which supply the eye.
- Causes:
- Carotid artery stenosis (most common)
- Cardioembolic sources also important cause.
Symptoms
- Sudden painless monocular vision loss
- May have some temporal sparing.
 Signs
Signs
- APD in affected eye
- Funduscopic exam: Whitening of ischemic inner retinal layers with sparing in the foveal region (which is supplied by the intact choroidal circulation) creating the classic “cherry-red spot”
Emergency Department Management
- Emergency ophthalmology consult, stroke work-up
- Treatment options
- No clinical trials have demonstrated improvement with any treatment compared with observation.
- Management options described in the literature
- Tissue plasminogen activator (tPA)
- Ocular massage
- Ocular pressure lowering agents / maneuvers
- Topical agents such as timolol
- IV agents such as acetazolamide or mannitol
- Anterior chamber paracentesis
- Vasodilatory Agents (nitroglycerin, pentoxifylline, isosorbide, carbogen, breathing into a bag – causes increase in CO2 leading to vasodilation)
Amaurosis Fugax (Bagheri 2015, Hayreh 2014, Pula 2016)
Definition: Sudden and transient visual loss or transient blurring or obscuration of vision, with normal recovery of vision after the episode. Can be all the visual field or just part of the visual field
- Comes from Greek terms “amauroun” (to darken) and the Latin “fugax” (fleeting)
- Should be distinguided from “transient vision loss (TVL). TVL is from an extra-ocular cause of vision loss (i.e., stroke) and amaurosis fugax is from an intraocular derrangement
Causes
- Carotid artery disease, (classic form)
- Embolic disease (CRVO, CRAO)
- Hypercoagulable state
- Retinal migraine
- Cocaine
- Inflammatory disease of the arteries (GCA)
Symptoms
- Painless unilateral vision loss, may be all visual field or part of visual field.
- “Curtain dropping over eye” that resolves over a few seconds to minutes
Signs
- Residual visual acuity deficit may be present
- Often have no abnormalities on ED evaluation
Emergency Deratment Management
- Investigate for potential embolic sources
- Ischemic stroke workup
- Ophthalmological and neurological consultation
- The time between an episode of amaurosis fugax and the occurrence of a subsequent vascular event (i.e. a CVA) varies from a few hours to several days
Take Home Points
- Suspect glaucoma in any patient with an acute change in vision and get an intraocular pressure measurement
- First line treatment in acute angle closure glaucoma is a topical beta blocker
- Consider giant cell arteritis in patients with unilateral headache, jaw claudication and change in vision
- Don’t wait for the biopsy to start steroids in giant cell arteritis as this therapy is vision saving
- Assess patients with floaters or flashers for retinal or vitreous detachment. Rapid diagnosis and emergency referral improves outcomes of ophthalmologic interventions
Read More
Bhatia K, Sharma R: Eye Emergencies in Adams J.G. et al, Emergency Medicine Clinical Essentials ed 2. Philadelphia: Elsevier, 2013 (Ch) 26: p. 209-225
Walker R, Adhikari S.: Eye Emergencies, in Tintinalli J et al (eds): Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, Seventh Edition New York City: McGraw-Hill 2016 (Ch) 241
Guluma K, Lee JE. Ophthalmology, in Marx J et al (eds): Rosens Emergency Medicine: Concepts and Practice, ed 9. Philadelphia: Elsevier, 2018 (Ch) 61: p. 790-819
EM docs: Central Retinal Artery Occlusion
CanadiEM: Medical Concepts – Acute Angle Closure Glaucoma
ALiEM: Ocular Ultrasound: Retinal Detachment and Posterior Vitreous Detachment
References
Bagheri N, Mehta S. Acute Vision Loss. Primary care. 2015; 42(3):347-61. PMID: 26319342
Weinreb RN et al. The pathophysiology and treatment of glaucoma: a review. JAMA. 2014; 311(18):1901-11 PMID: 24825645
Schmidl D et al. Pharmacotherapy of glaucoma. Journal of ocular pharmacology and therapeutics : the official journal of the Association for Ocular Pharmacology and Therapeutics. 2015; 31(2):63-77. PMID: 25587905
Hayreh SS. Ischemic optic neuropathy. Progress in retinal and eye research. 2009; 28(1):34-62. PMID: 19063989
Hollands H et al. Acute-onset floaters and flashes: is this patient at risk for retinal detachment? JAMA. 2009; 302(20):2243-9. PMID: 19934426
McAllister IL. Central retinal vein occlusion: a review. Clinical & experimental ophthalmology. 2012; 40(1):48-58. PMID: 22003973
Hayreh SS, Zimmerman MB. Amaurosis fugax in ocular vascular occlusive disorders: prevalence and pathogeneses. Retina (Philadelphia, Pa.). 2014; 34(1):115-22 PMID: 23632956
Pula JH, Kwan K, Yuen CA, Kattah JC. Update on the evaluation of transient vision loss. Clinical ophthalmology (Auckland, N.Z.). 2016; 10:297-303. PMID: 26929593

.JPG/image-full;max$643,0.ImageHandler){kind=link}