BACKGROUND:
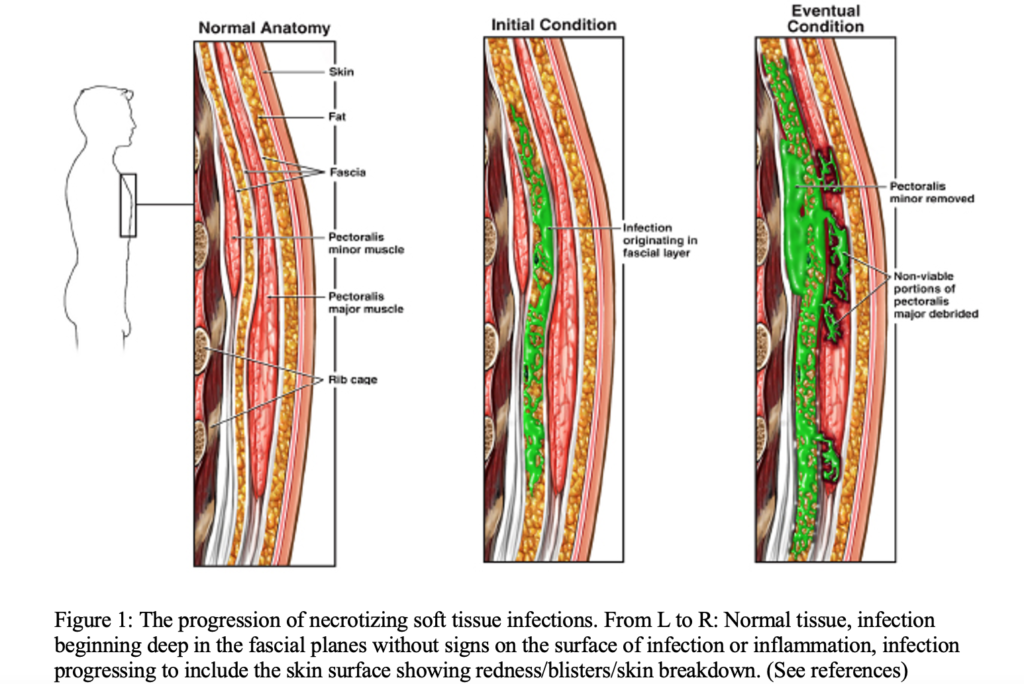
Necrotizing soft tissue infections are a rare but potentially lethal condition that can quickly lead to severe morbidity and mortality if not identified by clinical history and physical exam. It is a rapidly progressing infection that moves along fascial planes, often evading the immune system. This is a tricky diagnosis that can often be inconspicuous, so clinical gestalt is key. The definitive treatment of a necrotizing soft tissue infection is surgical debridement and removal of the necrotic tissue. Studies have shown that early surgical intervention is associated with reduced mortality, making early identification of this process very important.
While CT and MRI are commonly used imaging modalities for the evaluation of necrotizing soft tissue infections, they can be time consuming and potentially unsafe for an unstable patient. Point of care ultrasound (POCUS) can be a highly valuable tool for safe and rapid identification of necrotizing soft tissue infections.
EVALUATION:
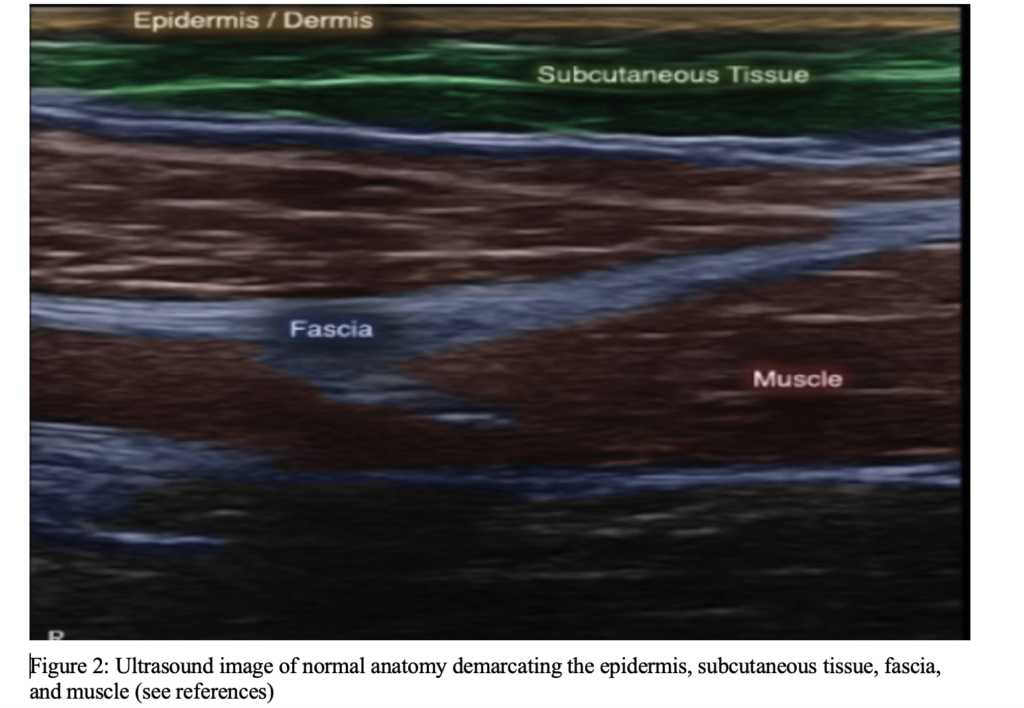
Scan the affected and contralateral body part for comparison with a sterile cover (or Tegaderm) overlying a high frequency linear probe.
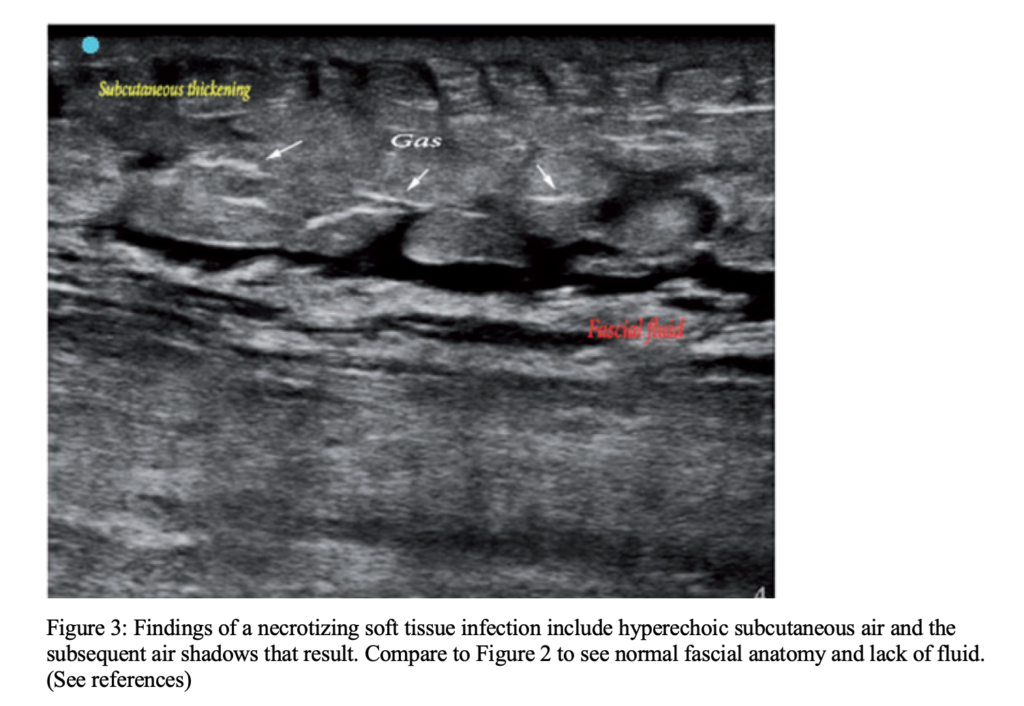
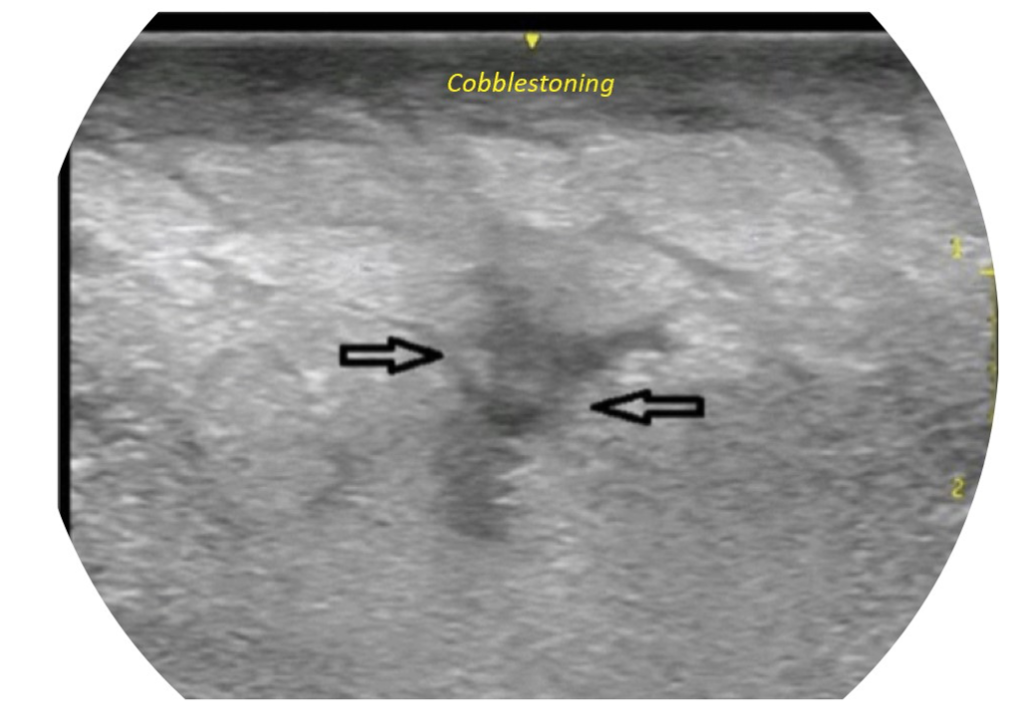
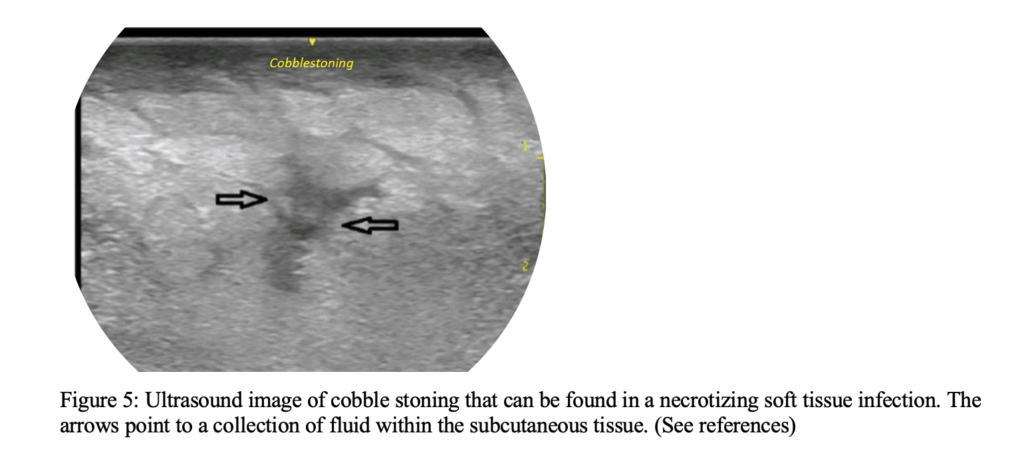
Ultrasound findings include STAFF:
- S/T for subcutaneous thickening
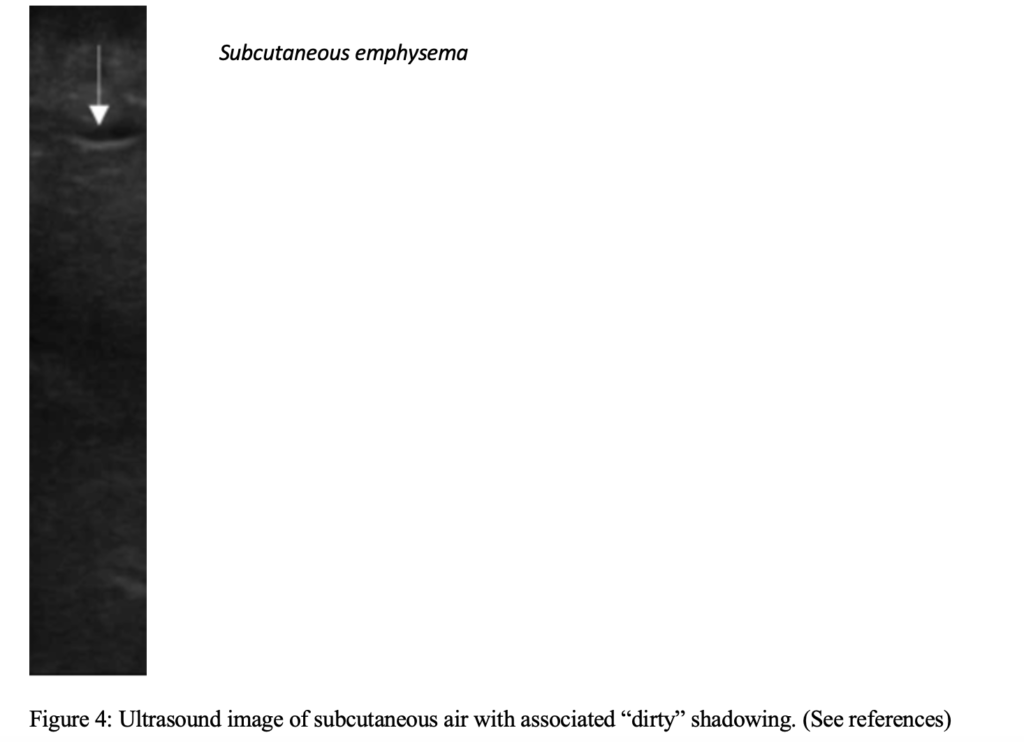
- A for air or emphysema in the subcutaneous tissue, which will appear as dirty shadowing – reverberation artifact from the interface where the air meets the tissue
- FF for a fascial fluid layer greater than or equal to 2 mm
Necrotizing soft tissue infections are diagnosed definitively via surgical exploration. However, the presence of these POCUS findings can prompt early surgical consultation and initiation of broad-spectrum antibiotics.
SUMMARY:
Upon initial evaluation of patients in the emergency department with clinical signs of soft tissue infections, consider using POCUS as a valuable tool to gather more information in patients with a high suspicion for the diagnosis and/or are too unstable to undergo CT imaging.
REFERENCES:
Castleberg E, Jenson N, Dinh VA. Diagnosis of necrotizing faciitis with bedside ultrasound: The staff exam. Western Journal of Emergency Medicine. 2014;15(1):111-113.
Clark ML, Fisher KL. Sonographic Detection of Necrotizing Fasciitis. Journal of Diagnostic Medical Sonography. 2017;33(4):311-316.
Joaquín Valle Alonso, Ganapathiram Lakshmanan, Yasser Saleem, Use of POCUS Ultrasound in sepsis, bedside diagnosis of necrotizing fasciitis, QJM: An International Journal of Medicine, Volume 110, Issue 10, October 2017, Pages 687–688.
Magalhães L, Martins SR, Nogué R. The role of point-of-care ultrasound in the diagnosis and management of necrotizing soft tissue infections. The Ultrasound Journal. 2020;12(1). doi:10.1186/s13089-020-0153-4
McHenry CR, Piotrowski JJ, Petrinic D, Malangoni MA. Determinants of mortality for necrotizing soft-tissue infections. Ann Surg 1995; 221:558–563.
Sarani B. Necrotizing fasciitis. Necrotizing Fasciitis. https://rarediseases.org/rare-diseases/necrotizing-fasciitis/. Published October 28, 2019. Accessed March 9, 2022.
VA; CEJND. Diagnosis of necrotizing fasciitis with bedside ultrasound: The staff exam. The western journal of emergency medicine. https://pubmed.ncbi.nlm.nih.gov/24578776/. Accessed February 28, 2022.
Voros D, Pissiotis C, Georgantas D, Katsaragakis S, Antoniou S, Papadimitriou J. Role of early and extensive surgery in the treatment of severe necrotizing soft tissue infection. Br J Surg 1993; 80:1190–1191.
Wallace HA, Perera TB. Necrotizing Fasciitis. [Updated 2021 Jul 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan.
Wronski M; Slodkowski M; Cebulski W; Karkocha D; Krasnodebski IW; Necrotizing fasciitis: Early sonographic diagnosis. Journal of clinical ultrasound: JCU.