
Traumatic Arthrotomy (forums.mtbr.com)
Definition: a deep laceration that extends into the joint capsule, exposing the intra-articular surface to the environment
- A laceration into the joint exposes the normally sterile intra-articular contents to external contamination
- Inoculation of the joint often results in septic arthritis
Epidemiology
- Knee joint the most commonly involved joint
- Mostly men aged 25-32 (Konda 2014)
History: Mechanisms that should raise suspicion for violation of the joint capsule include penetrating trauma (knives, sharp objects, gunshot), falls, or other high energy injuries
Physical Exam
- Laceration over joint which may be large or small
- Local wound exploration
- Usually sufficient for diagnosis
- Approach
- Inject wound with local anesthetic
- Irrigate wound with sterile saline
- Probe to bottom of wound with hemostat or q-tip
- Visualize bottom of wound
- Exam findings suspicious for joint capsule involvement:
-
- Air bubbles
- Extravasation of joint fluid – straw colored, viscous, sometimes oily in appearance
-

X-Ray: Elbow Traumatic Arthrotomy
Diagnostic testing
- Imaging
- X-ray
- Always obtain at least two views at right angles to each other (i.e. anteroposterior and lateral)
- May see foreign body in joint
- Can also see intra-articular air
- CT scan
- Intra-articular air visualized on CT (Konda 2013)
- May be up to 100% sensitive for joint violation
- Study limited by small numbers, inclusion bias + inadequate gold standard
- Could potentially be used instead of or, more likely, in addition to the slide load test in the appropriate clinical setting
- Intra-articular air visualized on CT (Konda 2013)
- X-ray

- Saline load test
- Standard tool for assessment of traumatic arthrotomy
- Particularly useful if physical examination equivocal or plain radiographs non-diagnostic
- Technique (Video)
- Perform arthrocentesis of the joint with a large bore needle (18-20 gauge)
- Sterile saline is injected into the joint while passive movement is applied to the joint
- The laceration site is watched for saline extravasation indicating communication between the joint and external environment
- Sensitivity ranges from 34%-99% depending on the study, joint, and the amount of saline used to load the joint (Browning 2016)
- Methylene blue
- Aids in distinguishing a true positive from additional bleeding from the wound
- Recent studies suggest that the addition of methylene blue does not increase sensitivity if a sufficient amount of saline is used (Metzger 2012)
- Volume of fluid injected
- Varies depending on the joint in which you are injecting
- Higher volumes increase sensitivity but also increase pain for the patient
|
Joint |
Volume of Saline |
Sensitivity |
|
|
Knee |
50 ml |
46% |
Keese 2007 |
|
194 ml |
95% |
||
|
Elbow |
20 ml |
86% |
Feathers 2011 |
|
40 ml |
95% |
||
|
Ankle |
7 ml |
50% |
Bariteau 2013 |
|
30 ml |
95% |
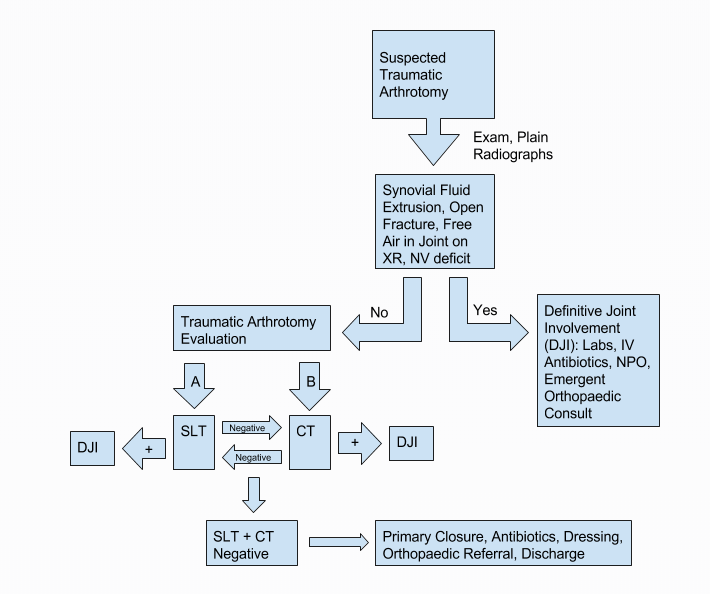
Traumatic Arthrotomy Workup Flow (epmonthly.com)
ED Management
- Reduce open fractures if present
- Irrigate grossly contaminated wounds in the ED
- Immobilize the joint to prevent further injury
- Obtain early orthopedic evaluation for joint exploration, and washout to be performed within 6-24 hours
- Tetanus prophylaxis
- Prophylactic antibiotics (best if given within 6 hours)
- Staph/strep coverage: 1st generation cephalosporin (i.e. cefazolin or cefuroxime)
- If risk factors for MRSA present, use agent with activity against MRSA (i.e. vancomycin)
- If significant soft tissue injury, add gram negative coverage like late generation cephalosporin, extended-spectrum penicillin, or aminoglycoside (i.e. gentamycin)
- If concern for fecal or clostridial infection, add high dose penicillin (i.e. zosyn)
- If seawater contamination and concern for vibrio vulnificus, add doxycycline
Prognosis
- Functional impairment correlates to the severity of injury
- Infection rate from periarticular wounds ranges from 0% to 11.8%
- Improved outcomes if diagnosis and treatment is achieved within 24 hours of injury (Konda 2014)
Take Home Points
- Always suspect an open joint if there is a laceration, regardless of size, the lies over joint
- Use the Ssaline load test to assess for joint capsule injury. Consider CT to assess for intraarticular air
- Obtain emergency orthopedics consultation for all open joints and administer antibiotics and update tetanus in all patients
Read More
- emDocs: Open joints – ED evaluation and management
- Wheeless’ Textbook of Orthopedics: Open joint injuries
- EP Monthly: How to confidently rule out traumatic arthrotomy of the knee
References
Bariteau JT et al. Evaluation of saline load test for simulated traumatic arthrotomies of the ankle. Injury 2013; 44: 1498–1501. PMID: 23490316
Browning BB et al. Does the saline load test still have a role in the orthopaedic world? A systematic review of the literature. Acta Orthop Traumatol Turc 2016; 50: 597-600. PMID: 27979366.
Feathers T et al. Effectiveness of the saline load test in diagnosis of traumatic elbow arthrotomies. J. Trauma 71 2011; E110–113. PMID: 21768902
Keese GR et al. The accuracy of the saline load test in the diagnosis of traumatic knee arthrotomies. J Orthop Trauma 2007; 21: 442–443. PMID: 17762473
Konda SR et al. Computed tomography scan to detect traumatic arthrotomies and identify periarticular wounds not requiring surgical intervention: an improvement over the saline load test. J. Orthop. Trauma 2013; 27: 498–504. PMID: 23287770
Konda SR et al. Open Knee Joint Injuries—an evidence-based approach to management. Bulletin of the Hospital for Joint Diseases 2014; 72: 61-9. PMID: 25150328
Makhni MC. Traumatic Arthrotomy. Orthopedic Emergencies 2017. Springer, Cham
Metzger et al. Sensitivity of the saline load test with and without methylene blue dye in the diagnosis of artificial traumatic knee arthrotomies. J Orthop Traum 2012; 26: 347–9. PMID: 22215059