Definition: Displacement of the mandibular condyle from the temporomandibular fossa.
Epidemiology:
- Anterior dislocations are most common
- Mechanism
- Atraumatic (most common) from extreme mouth opening (yawning, eating, dental procedure, etc).
- Traumatic: superior and posterior dislocations more common in trauma
- TMJ dislocations typically occur bilaterally.
Diagnosis:
- Diagnosis can be made based on clinical exam alone
- Physical exam
- Inability to close the mouth
- Garbled speech
- Drooling.
- Anterior dislocations: Palpation of the TMJ can reveal one or both of the condyles to be anteriorly displaced in front of the articular eminence.
- Imaging (X-ray or CT)
- Helpful when patient has subtle presentation
- Should be obtained in traumatic dislocations as concomitant fracture is common
Management
- Atraumatic TMJ dislocations are typically managed non-operatively with ED reduction
- Supportive Care
- Provide analgesia as needed
- Local anesthestic (2-3cc) can be injected into the TMJ space or directly into the lateral pterygoid muscle
- Consider procedural sedation as muscle spasm often limits success of reduction techniques
- Reduction Techniques
- Gag Technique
- Elicit a gag reflex using a tongue depressor
- This reflex inhibits the muscles of mouth closure, thereby potentially allowing the condyle to move downward past the anterior lip of the mandibular fossa and relocating posteriorly
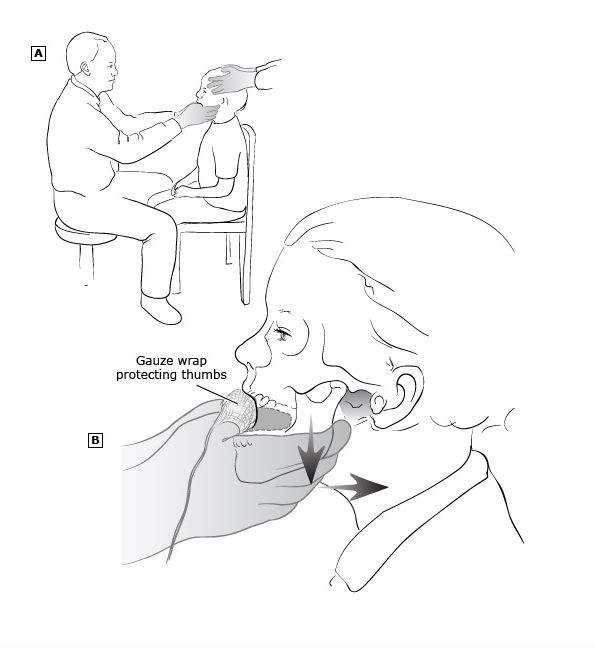
- Traditional (intraoral)
- Place the patient in an upright seated position
- While facing the patient, place bilateral thumbs (wrapped in gauze) on the inferior molars and the remainder of fingers around the outside of the jaw
- Apply downward and backward pressure to facilitate the condyles from the anterior aspect of the articular eminence
- Have another person hold the patient’s head to prevent movement
- This can also be done while standing behind and above the patient. You can use your abdomen brace the patient’s head
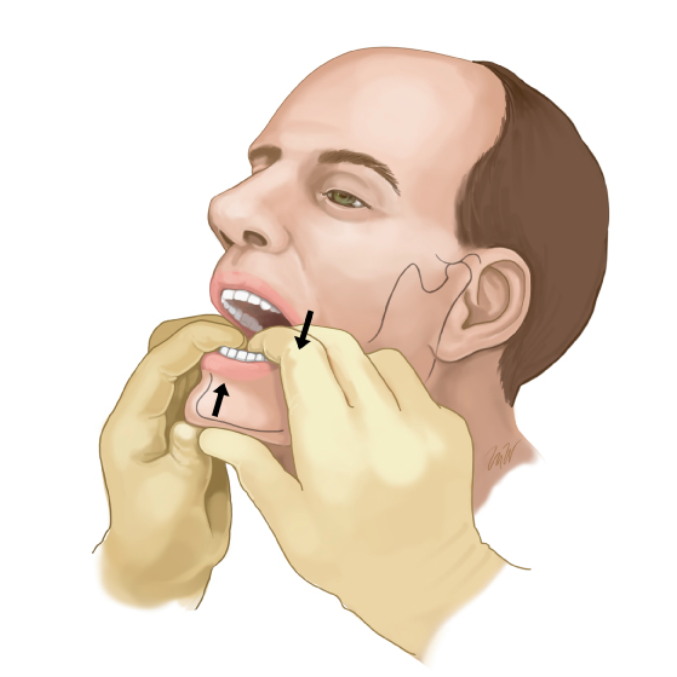
- Wrist pivot
- While facing the patient, grasp the mandible with both thumbs under the chin and place fingers on the occlusal surfaces of the lower molars
- Apply upward force with the thumbs and downward pressure with the fingers while pivoting the wrist forward
- Force must be equally applied to all sites to prevent fracture.
- Extraoral
- With one hand, grab the mandibular angle with fingers and place the thumb over the malar eminence of the maxilla
- With the other hand, place the thumb just over the displaced coronoid process and fingers behind the mastoid
- Simultaneously pull the mandibular angle forward on one side while pushing the coronoid process on the other causing one if not both TMJs to relocate back in the appropriate position
- Syringe Technique (Gorchynski 2014)
- Place a 5 or 10 cc syringe between the upper and inferior molars of the affected size
- Syringe size is determined by the mouth opening of the patient
- Instruct the patient to roll the syringe back and forth between the teeth, until reduction is achieved
- Success rate: 97% (30/31)
- Gag Technique
- Post-reduction Care
- Advise patient to avoid extreme mouth opening and to eat soft foods for 1 week
- Follow-up with ENT or oral surgery as needed
- Chronic dislocations may require surgical fixation

Take Home Points
- Atraumatic TMJ dislocations are typically anterior in nature and can be reduced by a variety of techniques in the ED
- Traumatic TMJ dislocations often involve mandible fractures and typically require open reduction and fixation in the operating room
- Consider using the syringe, gag and extraoral reduction techniques first line as they frequently do not require parenteral analgesics or procedural sedation
References:
Amsterdam JT: Oral Medicine, in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2010, (Ch) 70: p 895-909.
Gorchynski J et al. The “syringe” technique: a hands-free approach for the reduction of acute nontraumatic temporomandibulardislocations in the emergency department. J Emerg Med. 2014; 47(6):676-81. PMID 25278137
Marx JA et al. Rosen’s Emergency Medicine: Concepts and Clinical Practice, 7 ed. Philadelphia: Mosby Elsevier, 2010.
Mendez DR et al. Reduction of temporomandibular joint (TMJ) dislocations. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA.
Riviello RJ. Otolaryngologic Procedures. Roberts & Hedges’ Clinical Procedures in Emergency Medicine. Philadelphia: Elsevier Saunders, 2014. 6 ed. Ch 63: 1298-1341