Definition: Twisting of the spermatic cord leading to decreased blood flow to the testicle resulting in ischemia, infarction and potentially, tissue necrosis.
Epidemiology:
- Most common cause of acute scrotal pain in prepubertal boys
- Torsion present in 3.2% of all children presenting to the ED with scrotal pain (Ben-Israel 2010)
- Bimodal frequency: peaks in 1st year of life and again at puberty
- Risk factors: History of cryptorchidism, horizontal testicular lie, increased spermatic cord length
Pathophysiology: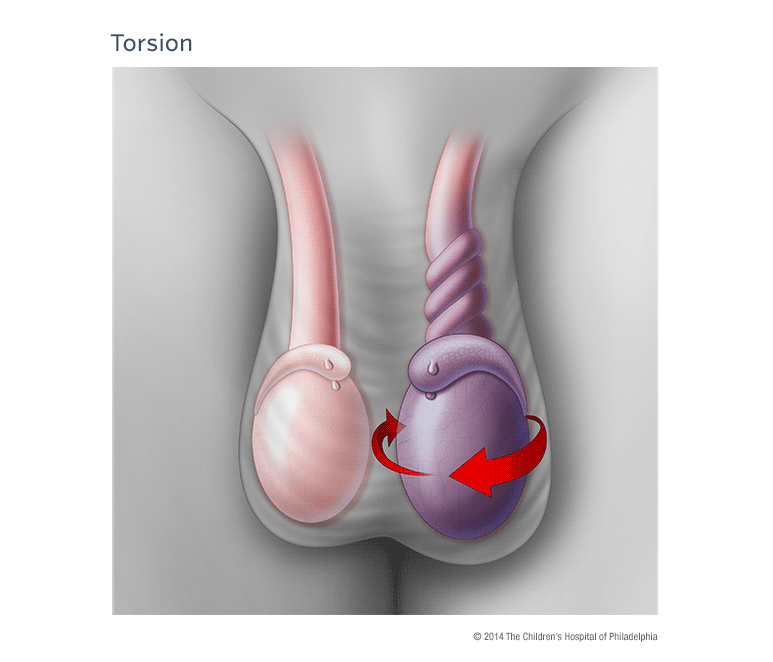
- Anatomical defect in the tunica vaginalis allowing the testicle to rotate when the cremasteric muscle contracts
- Twisting of the testicle initially causes compromised venous return and can lead to arterial obstruction, ischemia and tissue necrosis
- Testicle can rotate from 180o to 720o
- Longer duration of torsion increases the risk of tissue necrosis
- Torsion recognized within 6 hours has an 80-100% salvage rate
- Persistent symptoms > 24 hours has a nearly 0% salvage rate
Differential Diagnosis
- Hydrocele
- Epididymitis
- Epididymorchitis
- Trauma
- Inguinal hernia
- Testicular tumor
Clinical Presentation
“No discriminating features, in either history or examination conclusively differentiate the correct diagnosis”(Sidler 1997)
History
- Sudden onset of scrotal pain
- Up to 20% of patients will have abdominal or flank pain alone (Mellick 2012)
- Nausea and vomiting
- History of blunt trauma (~ 10% of patients)
- History of similar pain in the past
- Presentation is often delayed (mean time to presentation 9.5 hours) (Rosen’s)
- Duration of symptoms should NOT guide management
- Historically, believed that symptoms > 24 hours inconsistent with salvageable tissue
- However, testicle may torse + detorse making it difficult to know how long ischemia present
Physical Examination
- Unilateral tender, firm testicle
- Scrotal erythema, edema and swelling
- Affected testicle typically higher than the unaffected one. OR = 58.8 (Ben-Israel 2010)
- Loss of cremasteric reflex
- Previously thought to be 100% sensitive and highly specific
- 30% of males with normal testicles will have an absent cremasteric reflex
- Studies report varying sensitivities as low as 60% (Mellick 2012)
- Horizontal (instead of vertical) testicular lie
Diagnosis
- The diagnosis of testicular torsion should be pursued in any patient with acute scrotal pain. Physical exam, history and imaging all have significant limitations.
- In patients with a high suspicion for torsion, emergent surgical consultation should not be delayed by diagnostic imaging as “time is testicle”
- Scrotal Ultrasound
- Standard imaging technique
- Diagnostic characteristics
- Sensitivity: 88 – 100% (+ Lr = 8.8 – 10)
- Specificity: 90%
- (+) LR = 8.8-10, (-) LR = 0.13
- Findings
- A torsed testicle will be hypoechoic, heterogeneous and enlarged
- Color doppler will demonstrate decreased or absent blood flow
- A partially-torsed testicle may have arterial flow but no venous flow, or may show an abnormal high-resistance pattern of arterial flow
- A testicle that has recently de-torsed will appear enlarged and hyperemic
- Due to the relatively low sensitivity, a negative color doppler ultrasound does not always rule out the disease
- Examination of the spermatic cord for twisting increases the false negative rate improving the utility of ultrasound to rule out the diagnosis
Ultrasound Images of Torsion

Right Testicle with Decreased Flow on Color Doppler - www.ultrasoundcases.info

Right Testicle with Swelling and Decreased Flow on Color Doppler - Radiopaedia.com

Left Testicle Hypoechoic and Swollen - www.radiologyassistant.nl
Management:
- ALL patients with suspicion for testicular torsion should have immediate consultation with a urologist for potential operative exploration and repair.
- Establish IV access and provide analgesia
- Manual detorsion
- Can be attempted if urology consultation is not immediately available
- May be successful in 25-80% of testicular torsion cases (Rosen’s 2014)
- Procedure
- Place patient supine
- Provider stands at the patients feet
- Apply “open book” rotation: rotate affected testicle away from midline
- Rotation required may be anywhere from 180o – 720o
- Up to 1/3 of patients will be torsed in the “opposite” direction (Mellick 2012)
-
- Regardless of the success of manual detorsion, all patients will require surgical evaluation

Surgical Evaluation – www.sages.org
Take Home Points
- Consider the diagnosis of testicular torsion in all patients with acute testicular pain
- Testicular torsion is a surgical emergency that requires immediate urologic consultation to increase the rate of tissue salvage.
- History, physical examination and ultrasound are all flawed in making the diagnosis. The gold standard is surgical exploration
- Consider manual detorsion in patients where consultation will be delayed
References
Ben-Israel T et al. Clinical predictors for testicular torsion as seen in the pediatric ED. Am J Emerg Med 2010; 28:786-789. PMID: 20837255
Sidler D et al. A 25-year review of the acute scrotum in children. S Afr Med J. 1997;87(12) 1696-8. PMID: 9497837
Mellick LB. Torsion of the testicle: It is time to stopping tossing the dice. Pediatric Emer Care 2012; 28: 80-6. PMID: 22217895
Ban KM, Easter JS: Selected Urologic Problems; in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2014, (Ch) 99: p 1326-1356.
