Definition: Hyponatremia is defined as any serum sodium < 135 mEq/L. Severe symptomatic hyponatremia typically occurs at a serum sodium < 120 mEq/L though the rapidity of the change in sodium is a key factor in the development of symptoms
Causes of Hyponatremia
- Hypervolemic Hyponatremia: Total body sodium increased with a relatively larger increase in total body water
- Chronic renal failure
- Cirrhosis
- Heart failure
- Euvolemic Hyponatremia: Total body sodium normal but increased total body water
- SIADH
- Drug related: Diuretics, opioids, barbiturates, carbamazepine
- Psychogenic polydipsia
- Hypothyroidism
- Adrenal insufficiency
- Water intoxication
- SIADH
- Hypovolemic Hyponatremia: Both total body sodium and water are decreased but sodium to a greater extent
- Fluid loss: vomiting, diarrhea, sweating, GI suction
- Renal causes: salt-wasting nephropathies, renal tubular acidosis, mineralocroticoid deficiency, diuretics, osmotic diuresis
- Third spacing fluids: burns, rhabdomyolysis, bowel obstruction
- Dilutional Hyponatremia: Hyperglycemia (i.e. in DKA, Hyperosmolar hyperglycemic states)
- Pseudohyponatremia: hyperlipidemia, hyperproteinemia
Clinical Manifestations
- The clinical manifestations define the severity of the hyponatremia (i.e. the serum level does not define severity). Symptoms and signs are dependent on both the serum level as well as the rapidity of change in the serum sodium
- Mild/moderate Hyponatremia
- Headache
- Nausea/vomiting
- Muscle cramps
- Lethargy
- Restlessness
- Severe Hyponatemia
- Disorientation
- Focal neurologic deficits
- Seizures (Status epilepticus common)
- Coma
Diagnosis
- There are no classic physical exam or EKG findings (unlike in other electrolyte abnormalities) to use to clinch the diagnosis
- Due to vagueness of symptoms in mild/moderate hyponatremia and the non-specific nature of symptoms in severe hyponatremia, the diagnosis may be suspected but will be confirmed by obtaining a serum sodium level
- ALL patients with altered mental status, seizures or neurologic deficits should have their serum sodium level assessed
Management
- Supportive Care
- Judicious IV fluids: Only administer isotonic crystalloid if patient hypotensive
- Comatose patients may require airway management
- Status epilepticus
- Ensure that other reversible causes are managed (hypoglycemia, intracranial hemorrhage, hypoxia, hyperthermia etc)
- Consider RSI for airway protection
- Treat neurologic emergencies with hypertonic saline
- Rapid correction of serum sodium by 2-3 mEq/L typically results in correction of neurologic emergency (particularly status epilepticus)
- 3% Hypertonic saline
- 100-150 ml over 5-10 minutes. Can repeat bolus if needed
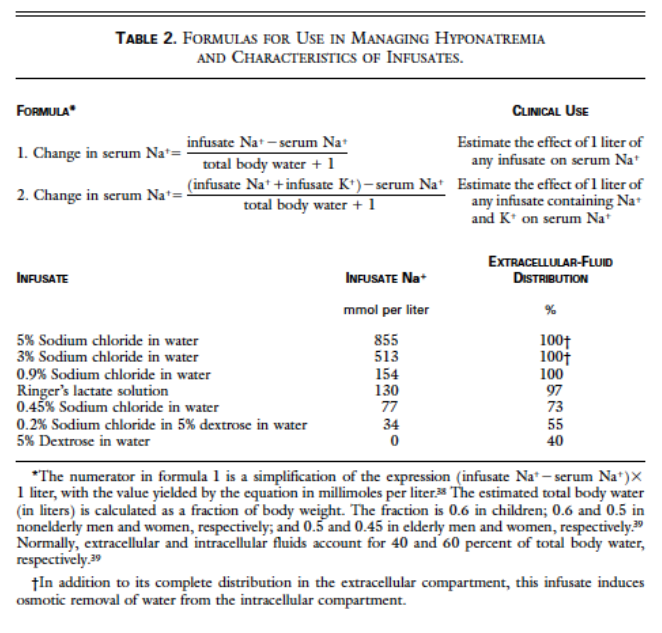 Alternate method: Androgue formula (Androgue 2000)
Alternate method: Androgue formula (Androgue 2000)
- Allows for use of multiple different hypertonic saline solutions in correction
- Formula may overestimate necessary volume for correction (Mohamand 2007)
- Alternate option: 50 cc of 8.4% sodium bicarbonate (1 “ampule” of crash cart bicarb)
- Goals of serum sodium correction
- 1st Hour: 1-3 mEq/L using bolus(es) of hypertonic saline
- 1st 24 Hours: 6-8 mEq/L (Sterns 2010)
- DANGER: Rapid Overcorrection
- Rapid overcorrection of serum sodium can cause osmotic demyelination syndrome (ODS)
- ODS can manifest as ataxia, quadraplegia, CN palsies or “locked-in” syndrome
- Can occur up to 7 days after rapid correction
- Preventing overcorrection
- Do not increase serum sodium by more than 6-8 mEqL in the 1st 24 hours
- Fluid restrict patient after relief of neurologic emergency
- Monitor urine output (UO): If UO > 100 ml/hr, send urine osmolarity + urine sodium
- Urine osmolarity < 100, give DDAVP 1 mcg
- Rapid overcorrection of serum sodium can cause osmotic demyelination syndrome (ODS)
- Correct Hypokalemia
- Often will see hypokalemia in patients with severe hyponatremia
- Correction of hypokalemia can improve hyponatremia
- Oral repletion safe and efficacious if patient tolerating oral intake
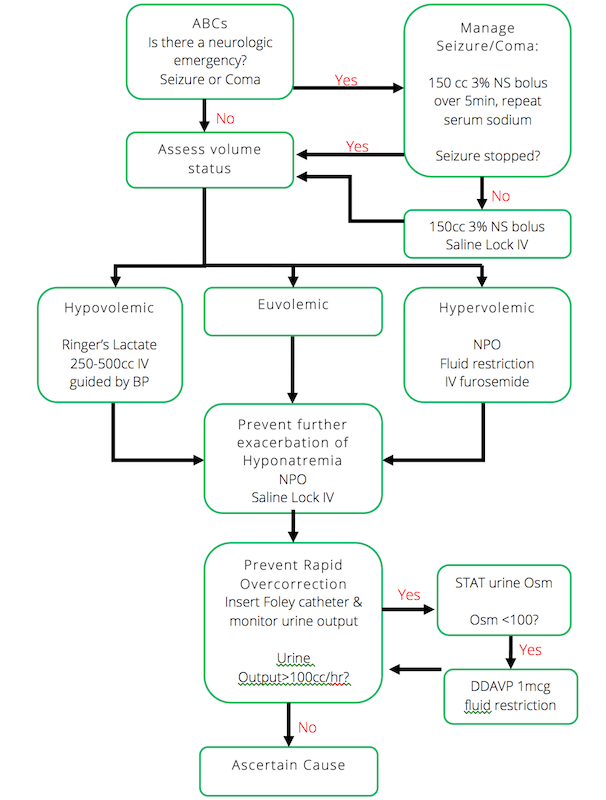
Hyponatremia Algorithm (EM Cases)
Take Home Points
- Severe hyponatremia is characterized by CNS dysfunction (focal neurologic deficit, seizures or coma) not by the serum sodium level
- Treat neurologic emergencies with 3% hypertonic saline. 100-150 ml of 3% hypertonic saline will raise the serum sodium by 1-3 mEq/L which typically will resolve neurologic emergencies
- Do not correct sodium by more than 6-8 mEq per day in order to avoid overcorrection and ODS
Read More
EM Cases: Podcast 60: Emergency Management of Hyponatremia
Pfenning CL, Slovis CM: Electrolyte Disorders; in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2014, (Ch) 125: p 1636-53.
References
Adrogue HJ, Maidas NE. Hyponatremia. NEJM 2000; 342(21): 1581-9. PMID: 10824078
Mohamand HK et al. Hypertonic saline for hyponatremia: risk of inadvertent overcorrection. Clin J Am Soc Nephrol 2007; 2: 1110-7. PMID: 17913972
Moritz ML, Ayus JC. 100 cc 3% sodium chloride bolus: a novel treatment for hyponatremic encephalopathy. Metab Brain Dis 2010; 25: 91-6. PMID: 20221678
Sterns RH et al. Treating profound hyponatremia: a strategy for controlled correction. Am J Kidney Dis 2010; 56: 774-9. PMID: 20709440

In hypovolaemic hyponataemia RL is potentially lethal brain cell expander.