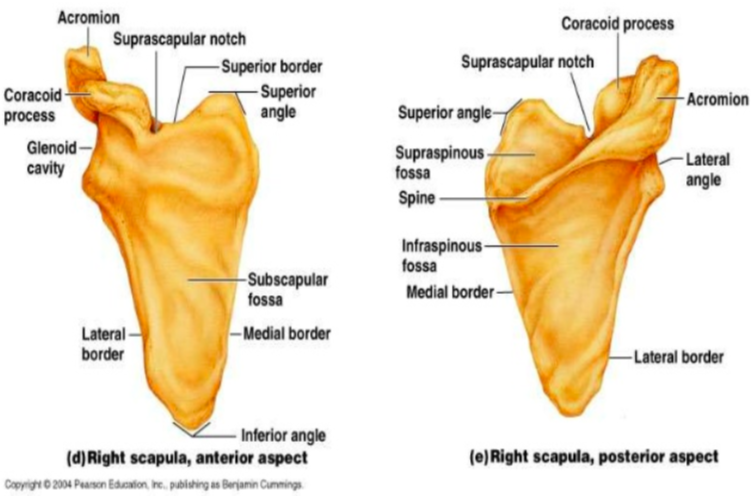
Anatomy
- Scapula does not have any bony connection to the thorax and serves primarily for muscle attachments
- Serves as origin for the deltoid muscle, providing leverage for the primary movements of the shoulder
Epidemiology (Wheeless 2018)
- Uncommon
- less than 1% of all fractures
- 3% of shoulder fractures (Murphy 2018)
- Fractures of the body and spine account for about 50% of scapular fractures
Mechanism of Injury
- Scapular fractures associated with high energy trauma
- MVCs account for 50% of scapular fractures (Murphy 2018)
- Falls from heights
- Direct trauma to shoulder
- Indirect trauma by FOOSH
- Non-accidental trauma in children
- Identification of scapular fracture should raise concern for further injury
Concomitant Injuries (Wheeless 2018)
- Concomitant injuries occur in 80-90% of patients
- 2-5% mortality rate, usually secondary to associated pulmonary or head trauma
- Associated with high Injury Severity Scores
- Associated Orthopedic Injuries
- Rib fractures (52%)
- Spine fracture (29%)
- Clavicle fracture (23%)
- Brachial plexus injury (5%)
- Associated Non-Orthopedic Injuries
- Pulmonary contusion (41%)
- Head injury (34%)
- Pneumothorax (23-32%)
- Vascular injury (11%), commonly axillary artery injury
- Association with blunt aortic injury may be overestimated
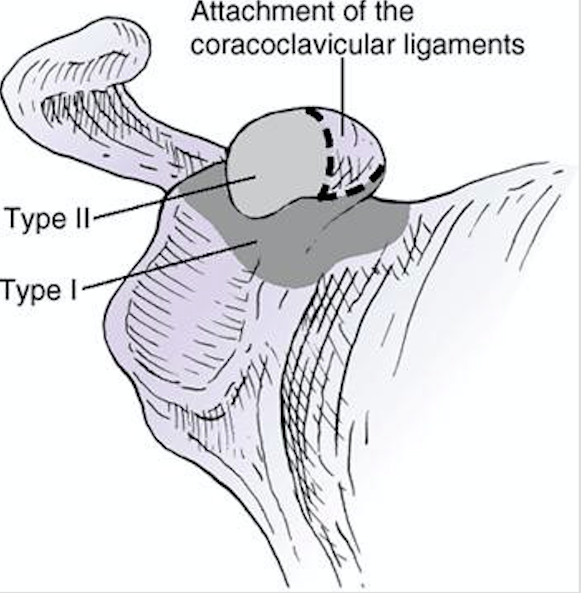
Glenoid Fractures (orthobullets.com)
Types of Scapular Fractures (Weatherford 2018)
- Scapular Body Fractures (~50%)
- Fractures described based on anatomic location
- Scapular Neck Fractures (~25%)
- Type I: Fracture of neck without associated clavicle fracture or AC joint dislocation
- Type II: Fracture of neck with associated clavicle fracture and AC joint separation
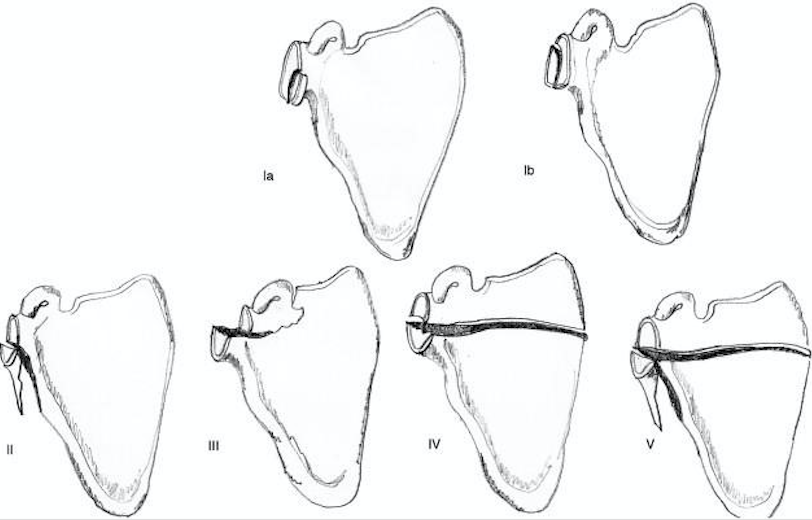
- Gelnoid Fractures (~10%)
- Type I
- Type Ia: Anterior rim fracture
- Type Ib: Posterior rim fracture
- Type II: Fracture line through glenoid fossa exiting scapula laterally
- Type III: Fracture line through glenoid fossa exiting scapula superiorly
- Type IV: Fracture line through glenoid fossa exiting scapula medially
- Type V
- Type Va: Combination of types II and IV
- Type Vb: Combination of types III and IV
- Type Vc: Combination of types II, III, and IV
- Type VI: Severe comminution
- Type I
-

Acromion Fractures (orthobullets.com)
Acromial Fractures (~ 8%)
- Type I: Nondisplaced or minimally displaced (IA: avulsion; IB: complete fracture)
- Type II: Displaced but does not reduce the subacromial space
- Type III: Displaced and reduces the subacromial space
- Coracoid Fractures (~ 7%)
- Type I: Displaced and reduces the subacromial space
- Type II: Fracture occurs toward the tip of the coracoid
Coracoid Fractures (orthobullets.com)

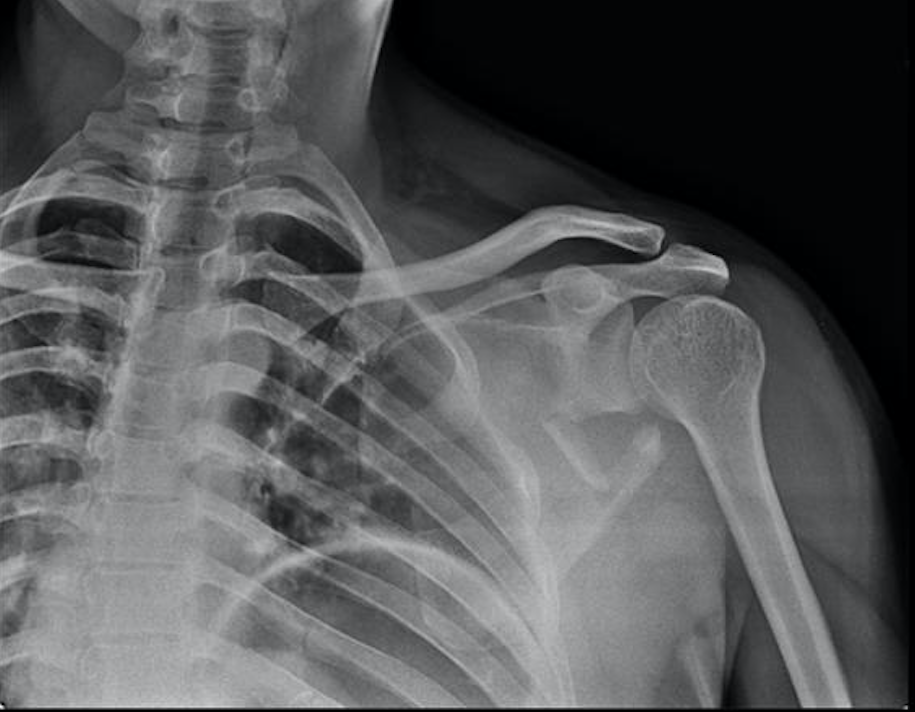
Scapula Body Fracture (Case courtesy of Mr Andrew Murphy, Radiopaedia.org. From the case rID: 45880)
Diagnostic Imaging
- Plain radiograph – recommended views
- True AP view of the scapula
- Lateral view
- Axillary view
- CT
- Obtain CT Chest in patients with scapular fracture following blunt chest trauma
- Standard for diagnosis and evaluation of the fracture and associated injuries
- Particularly useful in evaluation of intra-articular glenoid fractures
- 3D reconstruction can be helpful
Scapula Fractures (www.orthobullets.com)

Acromion Fracture (Case courtesy of Dr Maulik S Patel, Radiopaedia.org. From the case rID: 30094)

CT Scapula Body Fracture (Radiopaedia.org. From the case rID: 28072)