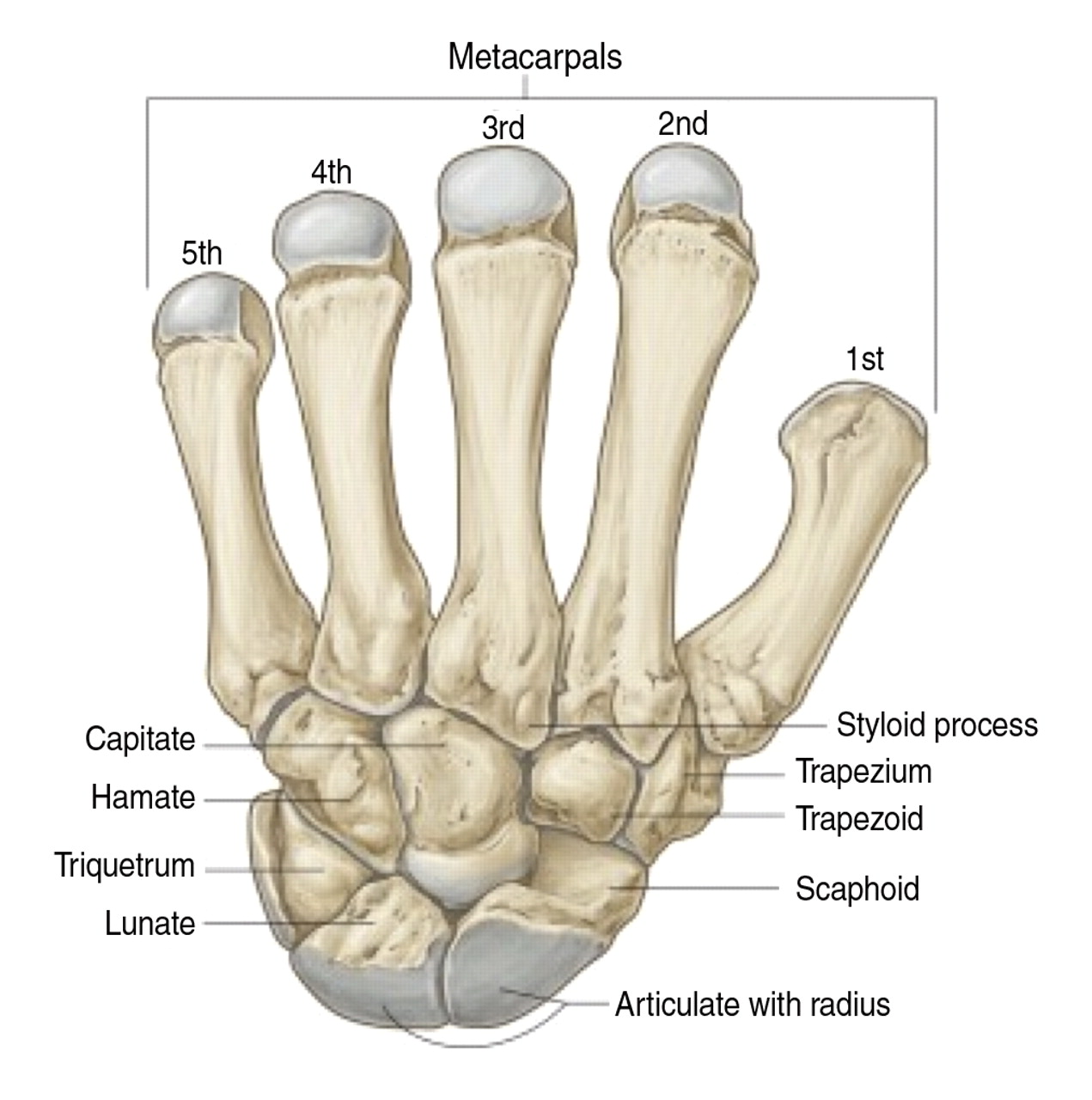
Carpal Bones (www.radiologictechnology.org)
Definition: Fracture of the scaphoid (navicular) bone, one of the carpal bones of the wrist
Epidemiology
- 10% of all hand fractures, 70% of all carpal fractures (Geissler 2001)
- Incidence of 12.3 in 100,000 each year in general population (Garala 2016)
Mechanism: results from axial load applied to a hyperextended and radially deviated wrist, most commonly after a fall on outstretched hand (FOOSH)
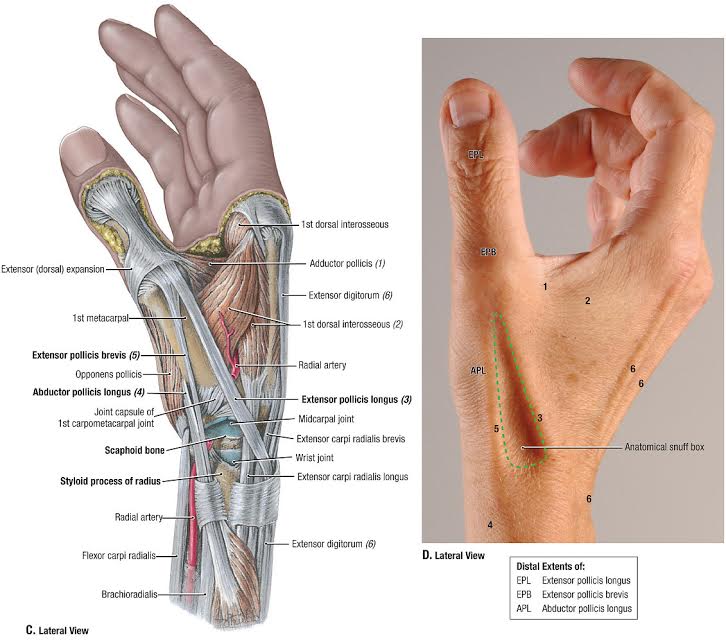
Anatomic Snuff Box (web.duke.edu/anatomy/lab11)
Physical Exam
- Anatomical snuffbox tenderness to palpation (Carpenter 2014)
- Presence of tenderness or pain with vibration, radial or ulnar deviation, or resisted supination do not significantly increase the likelihood of a scaphoid fracture
- Absence of anatomical snuffbox tenderness (LR-= 0.15) is predictive of absence of scaphoid fracture
- Absence of pain with resisted supination (LR-=0.09) is predictive of absence of scaphoid fracture
- Clamp sign
- (+) LR = 8.6
- (-) LR = 0.40
- When asked to indicate location of pain, patient forms a “C” with the opposite thumb and index finger and places around thumb
- Performance characteristics
- Resisted supination pain
- (+) LR = 6.1
- (-) LR = 0.09
- Resisted supination causes increased pain
- Performance characteristics

Physical Examination Test Characteristics (aliem.com)
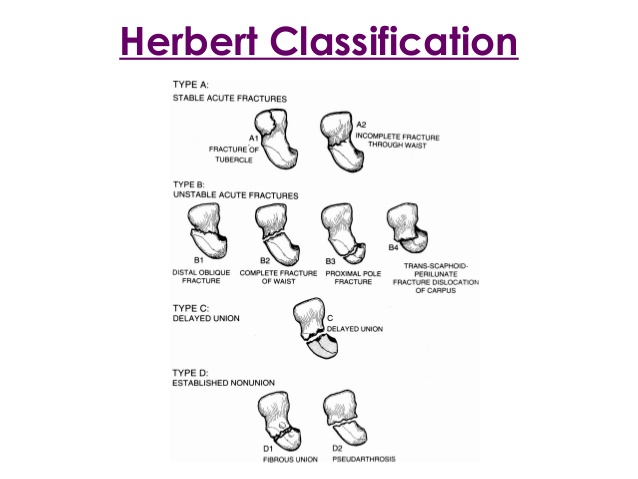
Herbert Classification System (image.slidesharecdn.com)
Classification Systems
Herbert Classification
- Based on stability of the fracture
- Unstable fractures
- Displacement of more than 1 mm or an angulation of more than 15 degrees between the fragments
- Additional carpal fractures, proximal pole fractures, multi-fragment fractures are also considered unstable (Rhemrev 2011)
Mayo Classification
- Classified by location of fracture site (Cooney 2013)
- Waist (middle 1/3) (80%)
- Distal (20%)
- Distal tubercle
- Distal articular surface
- Proximal (10%)
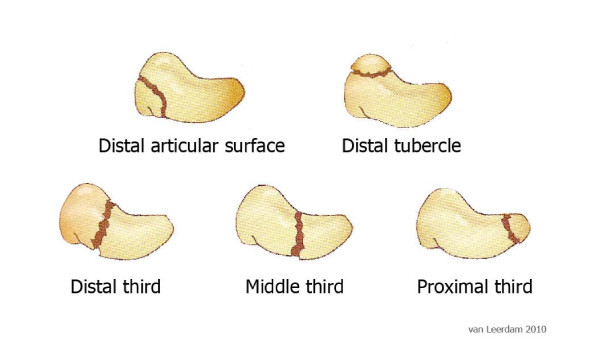
Mayo Classification System (www.researchgate.net)

X-ray with Scaphoid Fracture (noelhenley.com)
Imaging
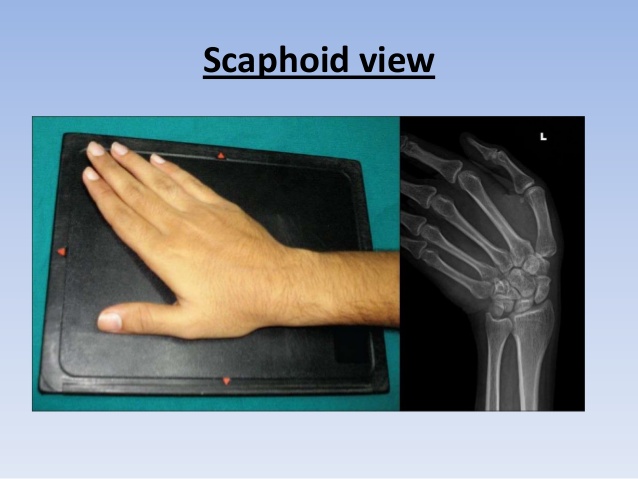
- For suspected scaphoid fractures, standard radiographs include posterior-anterior (PA), lateral, oblique and scaphoid views of the wrist
- Modified PA view obtained by positioning the wrist in 30 degrees extension and 20 degrees ulnar deviation.
- This view isolates the scaphoid from the superimposed shadow of the distal radius in the standard PA view (Insert SF 6)
- Scaphoid view:
- Up to 20% of scaphoid fractures may not be demonstrated on radiographs even with utilization of scaphoid view (occult fractures) (Waekerle 1987)
Scaphoid View (image.slidesharecdn.com)
-
Scapholunate Ligament Disruption (s-media-cache-ak0.pinimg.com)
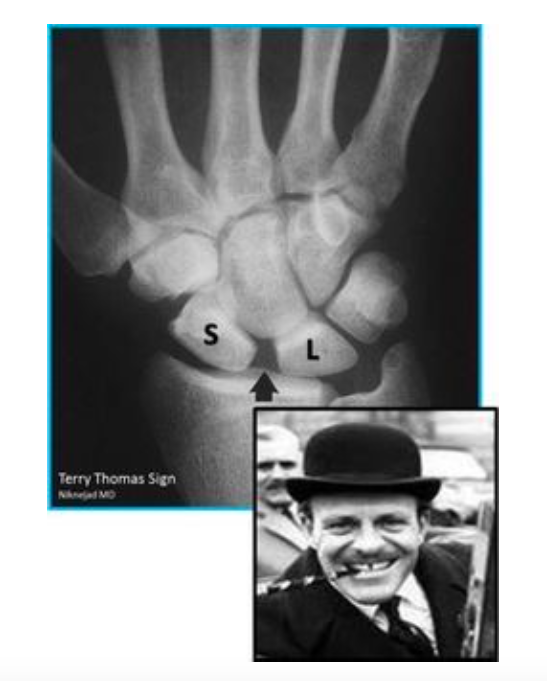
Associated scapholunate ligament disruption
- Suggested by >3 mm space widening between the scaphoid and lunate (also called “Terry Thomas” sign) and should be evaluated on every set of radiographs
- Unclear prevalence of concurrent injury with scaphoid fracture, however thought to be underestimated in the literature (Chun-Ying 2004)
- If clinical suspicion for scaphoid fracture is high with negative radiographs, advanced imaging techniques may be employed for diagnosis
- Sensitivity of 88 percent and specificity of 100 percent. It can also diagnose soft tissue injuries such as ligamentous damage (Mallee 2015)
- (+) LR = 22.0
- (-) LR = 0.09
- Most sensitive in the acute setting: < 24 hours post-injury
- Sensitivity = 72 percent
- Specificity = 99 percent
- (+) LR = 15.4
- (-) LR = 0.23
- MRI
- CT (Mallee 2015)
- CT and MRI can also evaluate degree of displacement and fracture pattern
- Bone scan has high sensitivity (99 percent), but found to have low specificity (86 percent) (Mallee 2015)
ED Management
- Non-displaced
- Patients should be placed in a short-arm thumb spica splint with the hand in “wine glass position” (slight dorsiflexion at wrist, digits in slight flexion)
- Follow-up with an orthopedist in 14 days for repeat x-rays and possible transition to cast
- Displaced or unstable fractures should be placed in a long arm thumb spica splint and referred to hand surgery follow-up as early as possible
- Due to high rate of false-negative x-rays in the immediate post-injury period, patients with snuffbox tenderness on exam or suspected fracture should be managed as having a non-displaced fracture due to significant complications that can occur
Avascular Necrosis of the Scaphoid Bone (www.guildfordupperlimb.co.uk)
Complications
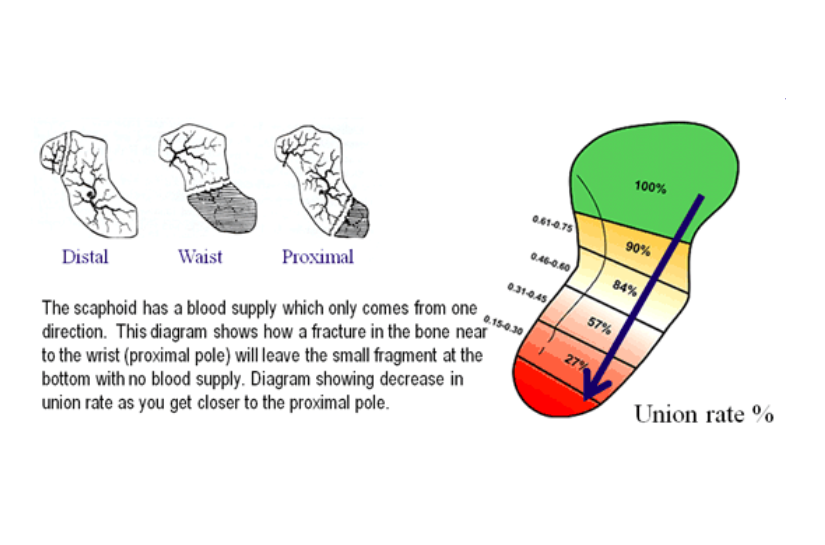
- Avascular necrosis
- The scaphoid blood supply comes from the dorsal branch of the radial artery coursing retrograde (proximal 80% of scaphoid) and superficial palmar arch (distal 20% of scaphoid).
- No direct blood supply to proximal portion of the bone
- Delayed union, malunion, or non-union are often associated with fractures that are inadequately immobilized
- Radiocarpal arthritis with associated wrist pain and stiffness
- Prevalence of up to 5% of scaphoid fractures even when correctly immobilized and healed (Lindström 1990)

Take Home Points
- The scaphoid is the most commonly fractured carpal bone. Always consider this injury in a patient with a fall on an outstretched hand
- Immediately after injury, as many as 20% of scaphoid fractures may be missed on x-ray even when dedicated scaphoid films are obtained
- Scaphoid fractures are a “can’t miss” ED diagnosis due to the high morbidity associated with their complications. Treat clinically suspected fractures (e.g. patients with snuffbox tenderness) as having non-displaced fractures, even in the setting of negative x-rays
Read More
ALiEM: PV Card Adult Scaphoid Fracture
ERCast: Splint Like a Pro – Thumb Spica Splint
Simon RR, Koenigsknecht SJ. Emergency orthopedics: The extremities. New York: McGraw-Hill 2011
References
Geissler WB. Carpal Fractures in Athletes. Clin Sports Med 2001; 20(1): 167-188. PMID: 11227704
Garala K et al. The epidemiology of fractures of the scaphoid: Impact of age, gender, deprivation and seasonality. Bone Joint J 2016; 98-B(5): 654-659. PMID: 27143737
Carpenter CR et al. Adult Scaphoid Fracture. Acad Emerg Med 2014; 21(2): 101-121. PMID: 24673666
Rhemrev SJ et al. Current methods of diagnosis and treatment of scaphoid fractures. Int J Emerg Med International J Emerg Med 2011; 4(1): 4. PMID: 21408000
Cooney WP. Scaphoid fractures: current treatments and techniques. Instr Course Lect. 2003;52:197–208 PMID: 12690849
Waeckerle JF. A prospective study identifying the sensitivity of radiographic findings and the efficacy of clinical findings in carpal navicular fractures. Ann Emerg Med 1987; 16(7): 733-737. PMID: 3592326
Chun-Ying C et al. Concurrent scaphoid fracture with scapholunate ligament rupture Acta Orthop Belg 2004; 70: 485-491 PMID: 15587040
Mallee WH et al. Computed tomography versus magnetic resonance imaging versus bone scintigraphy for clinically suspected scaphoid fractures in patients with negative plain radiographs. Cochrane Database Syst Rev. 2015 Jun 5;(6). PMID: 26045406
Lindström G, Nyström A. Incidence of post-traumatic arthrosis after primary healing of scaphoid fractures: a clinical and radiological study. J Hand Surg 1990; 15-B:11-13. PMID: 2307868
