Introduction
- Radial head subluxation (nursemaid’s elbow), is the most common elbow injury in children.
- Occurs mostly in children 1-4 years of age.
- Subluxation refers to a joint that is partially out of alignment.
- Dislocation refers to a joint that is completely out of alignment (Radial head dislocation occurs in the Monteggia fracture-dislocation)
- Mechanism involves traction of the arm at the wrist when
- A child is lifted by the wrist OR
- When a caregiver grabs the arm to prevent the child from falling or pulling away.
Anatomy
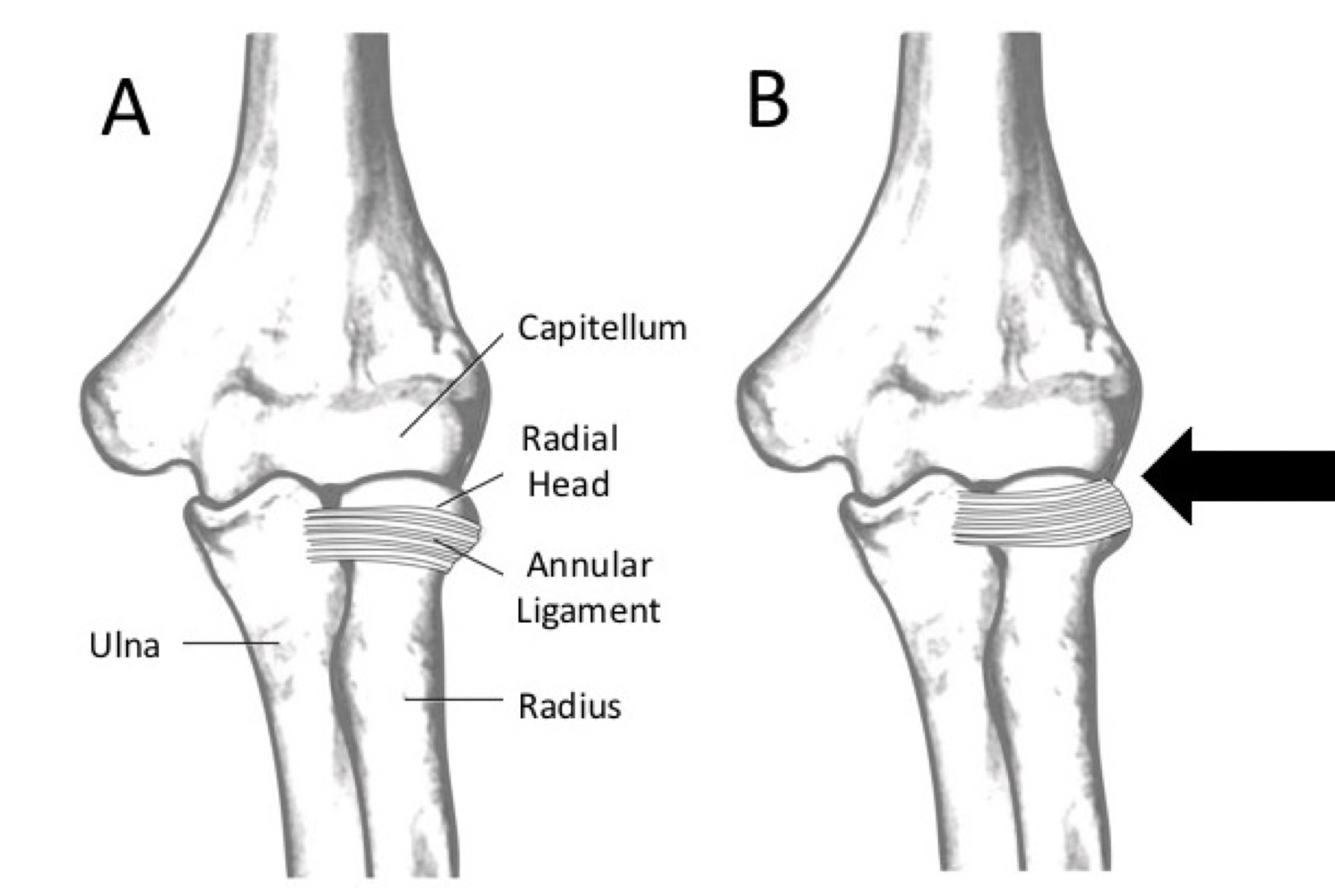
- The annular ligament secures the radial head to the ulna (A).
- In young children this ligament is loosely attached to the radius.
- With traction on the distal radius, a portion of the annular ligament slips over the head of the radius and slides into the radiohumeral joint where it becomes trapped (B).
- By 5 years of age the annular ligament has become thicker and tighter is less likely to be displaced.
Presentation
- The child will immediately complain of pain.
- Refuses to use the affected arm.
- The child is often in little distress unless attempts are made to move the elbow.
Examination
- It is best to have the patient sit on the parent’s lap with you sitting across from them
- Start by examining the unaffected arm in order to develop the patient’s trust and to establish a baseline for how they respond to your exam.
- Assess the neurovascular status of the injured arm.
- The neurovascular exam is challenging in young children and should be repeated, particularly after manipulation of the arm.
- Determine the degree of perfusion by palpating the radial and brachial pulses and assessing capillary refill, warmth and color in comparison to the unaffected limb.
- If a pulse is not palpable a Doppler ultrasound can be used to determine the presence of distal perfusion.
- Evaluate both the sensory and motor function of the ulnar, median and radial nerves while limiting movement of the elbow as this may precipitate or further exacerbate neurovascular injury.
- Orthopedics should be consulted in the patient with neurovascular compromise
- Identify gross deformity of the arm, such as the S-shape seen in severely displaced supracondylar fractures, or for any evidence of an open fracture, which may be as subtle as a small puncture wound at the site that the fractured bone poked through the skin.
- If radial head subluxation is suspected, examine the elbow last.
- The child with radial head subluxation typically holds the effected arm close to the body with the elbow slightly flexed and the forearm pronated. They will express pain or attempt to withdraw the arm with slight supination of the forearm.
- Palpate all bones starting from the medial clavicle and work distally. Take each joint gently through its range of motion.
Imaging
- The diagnosis of radial head subluxation is made clinically. If the history and physical are consistent with the classic mechanism for nursemaid’s elbow, X-RAYS are not necessary and a reduction maneuver can be attempted.
- When the mechanism involves significant trauma to the arm or the physical exam demonstrates any focal tenderness, deformity, swelling or neurovascular compromise then imaging is necessary prior to attempts at reduction.
Reduction Evidence
- Two maneuvers are typically used to reduce a radial head subluxation: the Supination/Flexion maneuver and the Hyperpronation maneuver (see below)
- A randomized clinical trial (Macias, Pediatrics 1998, PMID: 9651462) demonstrated that the hyperpronation technique required fewer attempts than the supination flexion method.
- A subsequent study (Green, Pediatric Emergency Care 2006, PMID: 16651912) revealed no difference in pain assessed by physicians but less pain in the hyperpronation group when assessed by nurses and parents.
Reduction Maneuvers
- Have the patient sit in a parent’s lap in a chair facing you.
- The parent’s arm can be used to hold the child across the chest and pin the unaffected arm to the side of the chest. The affected arm should be free.
- Hold the patients elbow with your arm that is on the same side as the patient’s affected arm (your right arm for their left arm or your left arm for their right arm)
- Place your thumb at the radiohumeral joint (at the junction of the radial head and the lateral epicondyle).
- Use your opposite arm to perform the maneuver (see below)
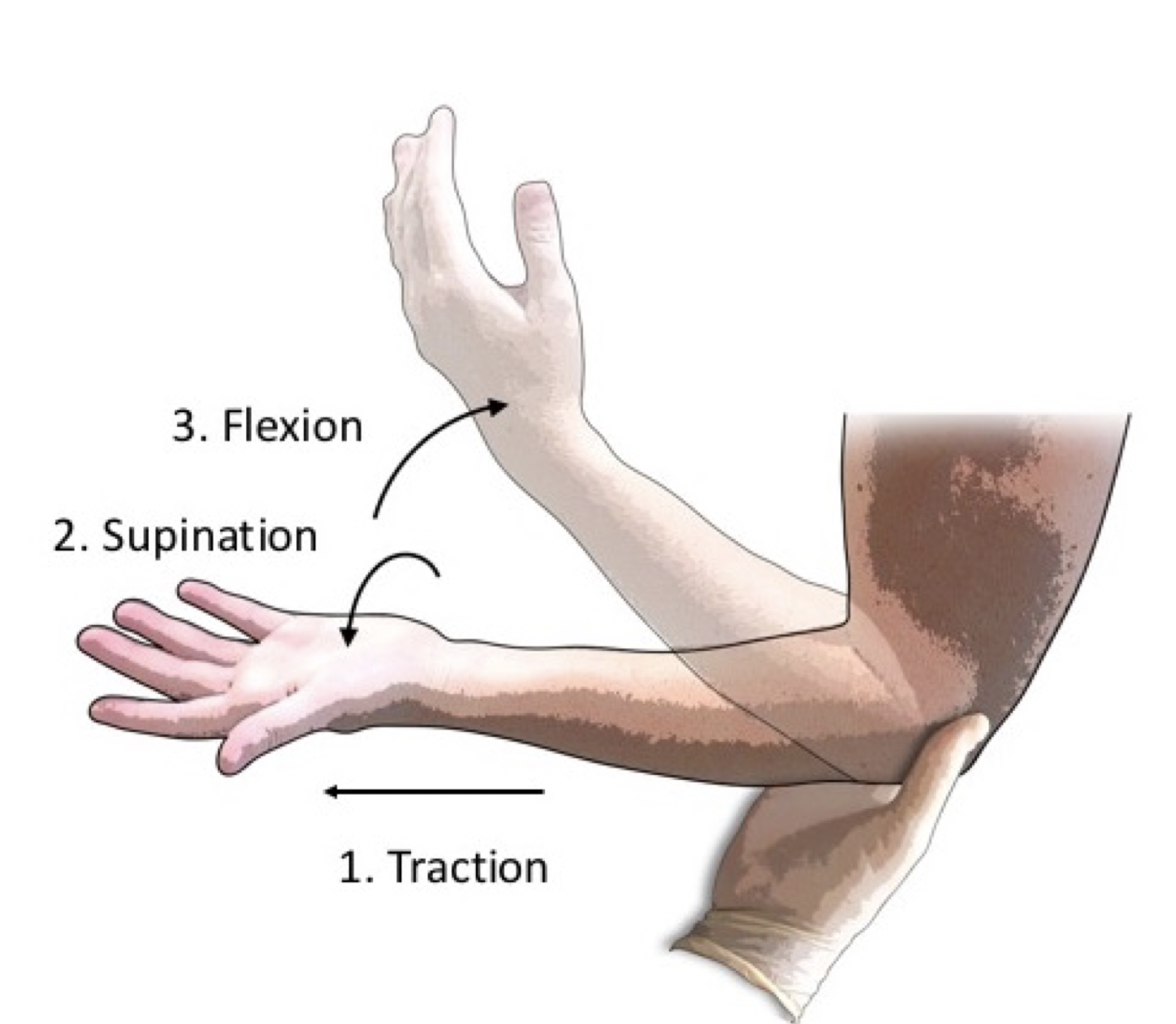
Supination / Flexion Method
- The provider supports the child’s arm at the elbow with one hand placing your thumb at the radio-humeral joint.
- The provider uses their other arm to hold the child’s distal forearm and applies gentle traction.
- While maintaining slight traction, the examiner supinates the child’s forearm fully and then flexes the elbow fully in one smooth motion.
- You may palpate a “click” or “clunk” at the radiohumeral joint as the radial head relocates
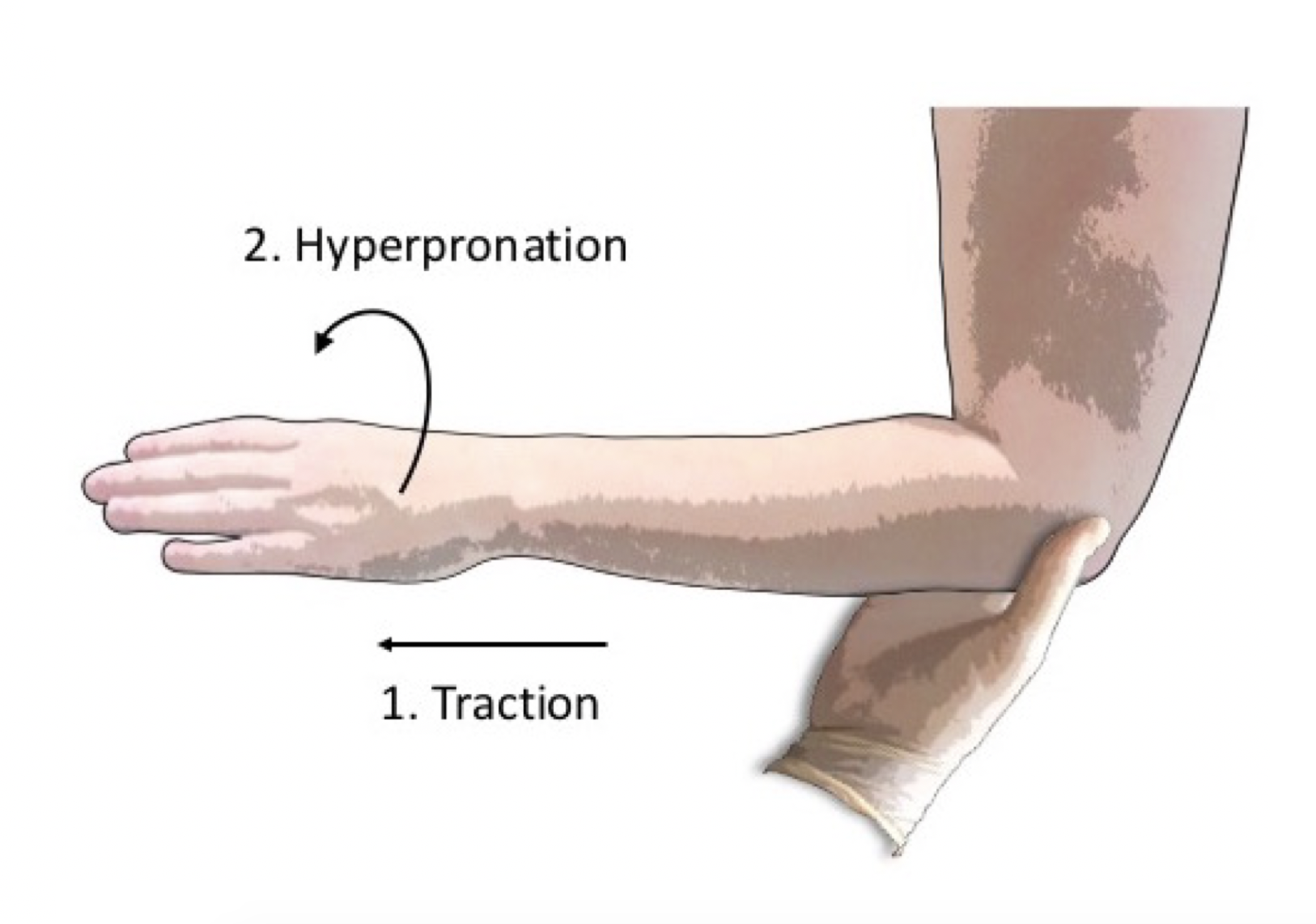
Hyper-pronation Method
- The provider supports the child’s arm at the elbow with one hand placing your thumb at the radiohumeral joint
- The examiner holds the child’s distal forearm with the other hand and hyperpronates the forearm while applying slight traction.
- You may palpate a “click” or “clunk” at the radiohumeral joint as the radial head relocates.
NOTE: The images above demonstrate each maneuver with the caregiver using their right hand to hold the patient’s left elbow. Note that the caregiver’s thumb is at the radiohumeral joint in order to feel the subtle “click” or “clunk” that occurs with relocation. Apply traction to the distal forearm to avoid twisting of the hand or wrist.
Post-Reduction Evaluation
- After the maneuver it may take some time for the child to realize that there is no longer any pain and begin to use the arm.
- If the attempt at reduction was successful, the child will begin to use the arm. If they can reach for an object above their head the reduction was successful.
- My trick to speed up the process is to stand with the child standing on the floor with the parents standing a few feet ahead of you. When you release the child, they will run to the parents and lift both arms above their heads to be picked up (to escape from the scary provider).
- Alternatively, have them go play in a quiet space where they can’t see you and wait until they start using the arm. Toys attached to the wall are great for this.
- If the first attempt was unsuccessful at reduction, either make a second attempt with the same maneuver or switch to the alternative maneuver.
- If multiple attempts are not successful an XRAY or orthopedic consultation may be warranted.
Discharge Instructions
- Radial head subluxation tends to recur because the annular ligament has stretched in the subluxation process. The parents should be educated to avoid traction on the arm.
Fantastic clear instruction!