Definition: Prolonged, pathologic erection of the penis for > 4 hours in the absence of sexual desire. There will be dorsal penile erection with ventral flaccidity resulting from engorgeent of the dorsal corpora cavernosa.
Pathophysiology
- Low-flow priapism
- Decreased venous outflow results in increased cavernosal pressure
- When cavernosal pressure exceeds arterial pressure, ischemia develops
- More common than high-flow version
- Typically accompanied by significant pain due to ischemia (can be considered to be compartment syndrome of the penis)
- Common causes
- Pediatric: Sickle cell disease, leukemia
- Adult: Intercavernosal injection (papaverine, phentolamine, PGE1), Anticoagulation, Pharmaceuticals (SSRIs, sedative-hypnotics, erectile dysfunction medications), Illicit drugs (cocaine, extasy)
- High-flow priapism
- Excess arterial inflow resulting in priapism
- Often painless
- Common causes
- Arterial laceration
- Spinal trauma
- Complications
- Penile fibrosis
- Urinary retention
- Incontinence
- Thrombosis + Ischemia (resulting from blood stagnation)
Differential Diagnosis
- Normal sexual arousal
- Penile trauma
- Urethral foreign bodies
- Spinal cord injury
- Peyronie’s disease
- Penile implant
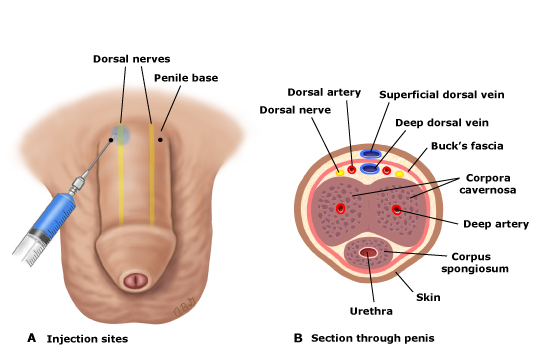
Dorsal Penile Nerve Block
Management
Basics:
- Low-flow or ischemic priapism is an emergency and prompt resolution is vital in avoiding complications
- Hydration may decrease sludging of blood if present
- Analgesia
- Systemic analgesia may not be effective
- Consider a dorsal penile block
- Easily performed both by landmark technique as well as US guided
- Block will facilitate further management
- Ultrasound guided block
- Relief of urinary obstruction
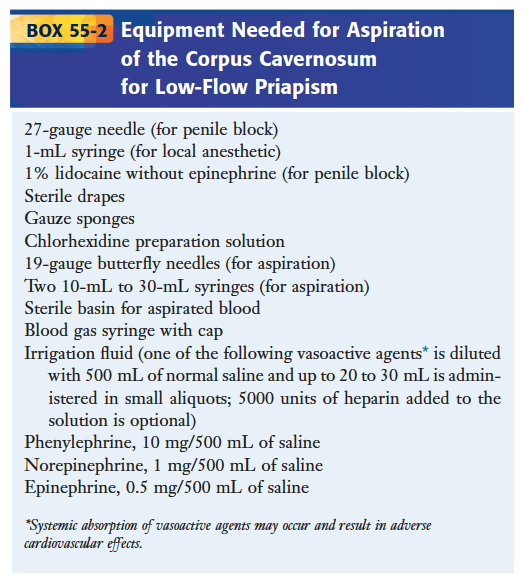
Aspiration + Irrigation Necessary Equipment (Roberts + Hedges’)
Directed Management
- Expeditious relief of priapism is centrally important. Ongoing ischemia compromises tissue leading to complications including fibrosis and impotence
- Non-invasive Management
- Warm compresses: Vasodilation leading to improved blood flow
- Terbutaline
- Mechanism of action: beta-2 agonist. Increases venous outflow
- Dose
- Oral: 5-10 mg
- Subcutaneous: 0.25-0.5 mg
- May repeat once after 15 minutes if no effect
- Unproven benefit of treatment (Govier 1994, Priyadarshi 2004)
- Should not delay definitive intervention
- Limited adverse effects
- Can be given while setting up for aspiration and irrigation
- Exchange transfusion
- Recommended in past for sickle cell patients with priapism but benefit unknown and potential for harm (ASPEN syndrome)
- Partial exchange transfusion (lower target hemoglobin) has also been recommended
- Consult hematology for assistance
-
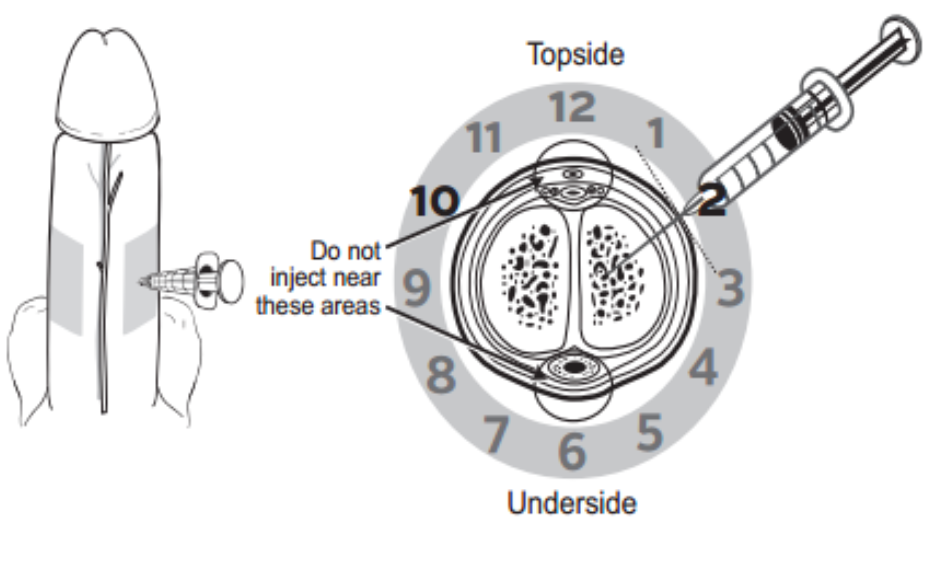
Intracorporal Injection (www.mskcc.org)
Invasive Management
- Intracorporal Injection
- Injection of alpha-adrenergic receptor agonists may cause cavernous smooth muscle contraction allowing for venous outflow
- Agents
- Phenylephrine
- Dose: 200 – 500 mcg (diluted in 1 ml of NS) intracorporal
- Can repeat injection q20 minutes up to 3 attempts
- Preferred due to low risk of CV side effects
- Epinephrine
- Dose: 100 mcg (diluted in 1 ml NS) intracorporal
- CV side effects including HTN and dysrhythmias are potential side effects
- Phenylephrine
- Technique
- Prepare skin in typical sterile fashion
- Insert 25- or 27-gauge needle at either the “10 o’clock” or “2 o’clock” position at the base of the penis
- Aspirate blood to confirm position
- Inject solution
- Bilateral injection not necessary as the copora cavernosa communicate
- Repeat injection in 30 minutes up to a total of 3 injections
- Aspiration and Irrigation
- Usually represents definitive management
- Prepare skin in typical sterile fashion
- Aspiration
- Insert 19-gauge “butterfly” needle into corpus cavernosa at “10 o’clock” or “2 o’clock” position
- Puncture site may be anywhere along corpus cavernosa (do not puncture glans)
- Advance needle at 45 degree angle to skin while drawing back on syringe until blood is returned (should be almost immediate)
- Continue aspirating until either bright red (arterial) blood returns or detumescence is achieved
- If successful, can consider instillation of vasoactive substance (Phenylephrine 200-500 mcg or Epinephrine 100 mcg as above)
- Tips
- Use small syringe (10 ml) as high level negative pressure can stop aspiration
- Access one corpus cavernosa only as the two bodies communicate
- Irrigation
- Should be employed if inadequate blood returns on aspiration or detumescence is not achieved
- Can be performed with or without vasoactive substance but solution containing vasoactive solution most frequently recommended
- Vasoactive solution
- Phenylephrine (preferred): 20 mcg/ml solution (1 mg phenylephrine in 500 ml NS)
- Epinephrine: 1 mcg/ml solution (1 mg epinephrine in 1000 ml NS)
- Inject 20-30 ml into the cavernosa, withdraw and discard
- Repeat until volume completed
- Complications
- Hematoma and infection are uncommon when proper precautions are taken
- Systemic circulation of vasoactive medications
- Place patient on cardiac monitor and check blood pressure frequently
- Epinephrine has higher risk for CV complications
- Successful Detumescence
- Place compressive elastic bandage (not too tight)
- Consider 3-day course of oral alpha-adrenergic agent (i.e. pseudophedrine)
- Urology follow up
- Intracorporal Injection
- Consult urology if none of the above techniques are unsuccessful for possible shunt placement
Take Home Points
- Priapism is compartment syndrome of the penis. Ischemia and infarction can occur with prolonged priapism and rapid treatment and detumescence is critical
- Provide adequate analgesia early to facilitate necessary interventions. Dorsal block of the penis is the most effective analgesic approach
- Do not delay aspiration and irrigation if more conservative measures fail as complications (fibrosis, impotence) can occur
Read More
McCollough M, Sharieff GQ: Genitourinary and Renal Tract Disorders; in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2014, (Ch) 174: p 2205-2223.
Davis JE, Silverman MA. Urologic Procedures; in Roberts JR: Roberts and Hedges’ Clinical Procedures in Emergency Medicine, ed 6. 2014, (Ch) 55: p 1113-1154

Complications of HiFlow must surely read incontinence and not incompetence?
Fixed. Thanks!
this was great… helped me do my first priapism drainage..!