INTRODUCTION
- Glomerulonephritis occurring days to weeks after preceding infection
- Often but not always group A Strep pharyngitis or impetigo
- Often affects children aged 3-12 but can occur in teens and adults
PATHOPHYSIOLOGY
- Antigen deposition in glomeruli → Interaction of antibodies in situ with antigens → Circulation of immune complexes → Deposition in glomeruli, with immune complex-mediated inflammation
CLINICAL MANIFESTATIONS
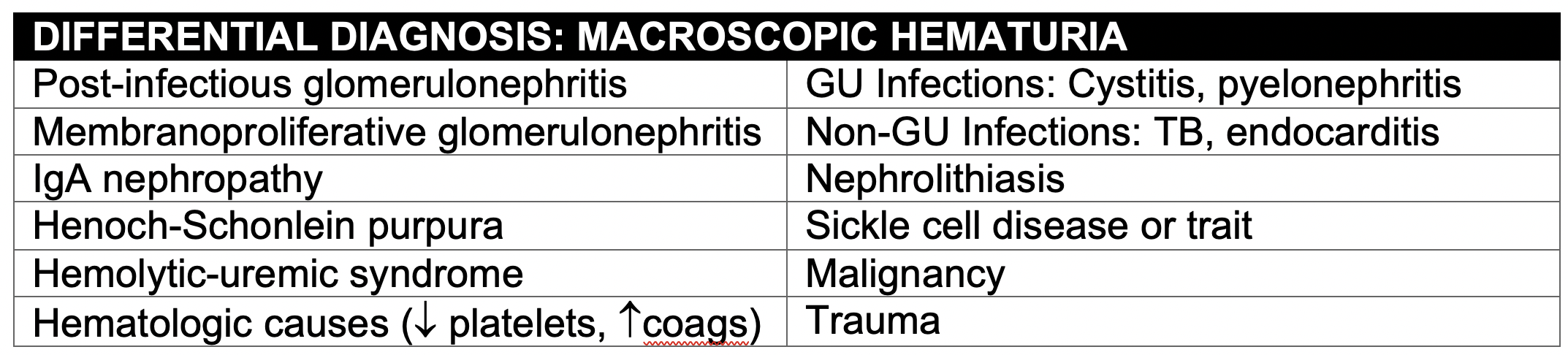
- Spectrum of severity, from asymptomatic hematuria to florid renal failure and acute nephrotic syndrome
- Gross hematuria is tea- or cola-colored; bright red blood indicates urinary tract bleeding
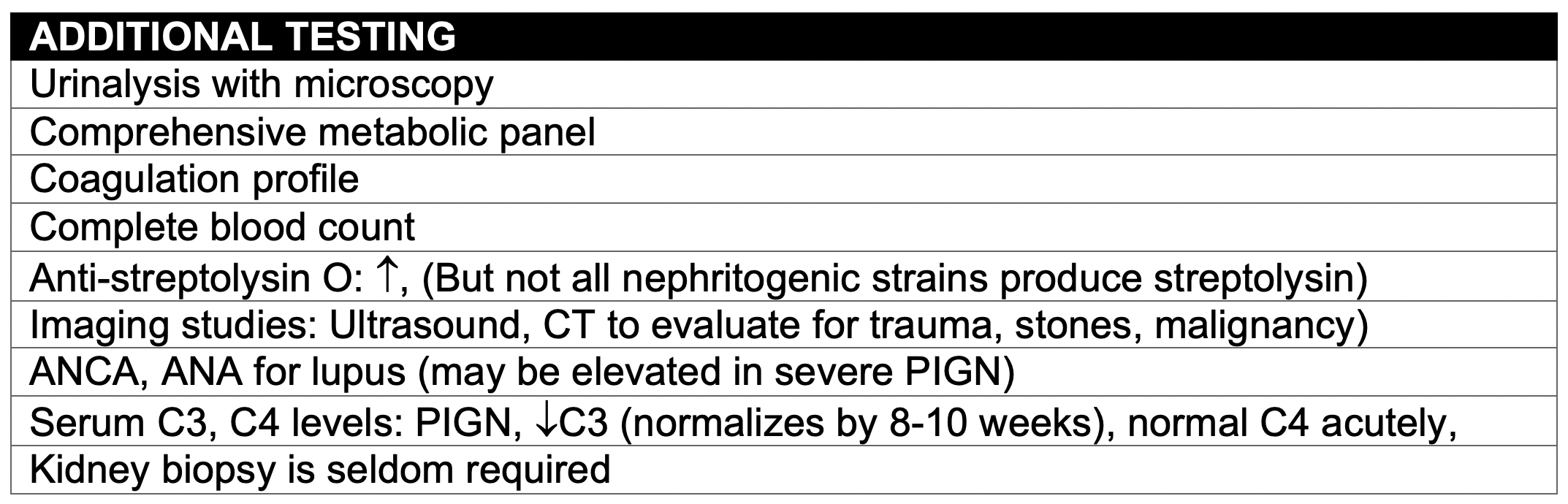
- Microscopy will differentiate true hematuria from dark urine caused by hemoglobin, myoglobin, or hypochlorite
- Seizure due to severe hypertension
MANAGEMENT
- No specific treatment
- Symptomatic treatment for:
- Volume overload: Water restriction, diuretics
- Hypertension: Antihypertensives (PO vs IV depending on severity and presence/absence of hypertensive urgency/emergency)
- Avoid ACE inhibitors, which can cause hyperkalemia
- Pulmonary edema: Diuretics, respiratory support
- Indications for Dialysis
- Life-threatening fluid overload refractory to therapy
- Hyperkalemia > 6.5
- Uremia with BUN > 89-100 mg/dL
PROGNOSIS
- Prognosis is generally good
- Hematuria usually resolves within 3-6 months; proteinuria takes longer to resolve
- If C3 levels do not normalize by 10 weeks or serum creatinine remains elevated or worsens, other causes of hematuria should be considered
- Long-term complications are rare but include hypertension or renal insufficiency years or decades after initial illness
