Pacemaker Terminology
- Five letter code system that describes the different pacemaker settings
- First three letters are most useful in ED management
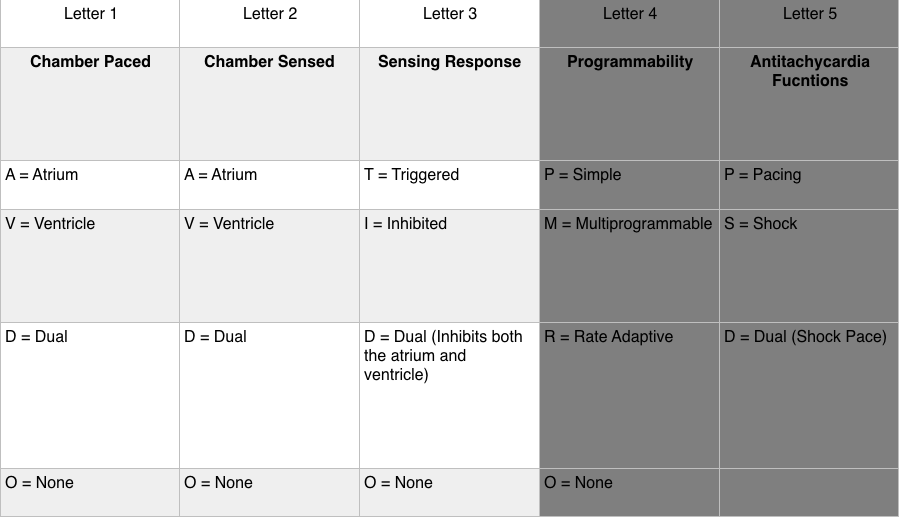
- Sensing Response
- Triggered (T): Sensed intrinsic depolarization will result in the pacemaker discharging (this setting not used in current generation pacemakers)
- Inhibited (I): Sensed intrinsic depolarization will result in inhibition of the pacemaker
- Dual (D): Dual inhibition of both atrial and ventricular pacing in response to intrinsic ventricular depolarization
- None (O): Does not trigger or inhibit regardless of the native activity
- Example #1: DDD
- Chamber paced: Atrium and ventricle can be paced
- Chamber sensed: Intrinsic depolarization of the atrium and ventricle is sensed
- Sensory response: Can inhibit pacemaker in response to an intrinsic ventricular depolarization OR trigger pacemaker in response to an atrial intrinsic depolarization with no associated ventricular response
- Example #2: VVI
- Device has a single lead in the ventricle that senses ventricular activity and can pace the ventricle
- An atrial event outside the refractory period will be inhibited
Common Indications for Permanent Pacemaker Placement
- Sinus node dysfunction: symptomatic sinus bradycardia, frequent/prolonged sinus pauses, impaired response to demand/exercise
- 3rd degree or advanced 2nd degree (Mobitz II) AV block with any of the following
- Symptomatic bradycardia
- Ventricular dysrhythmia resulting from AV block
- Symptomatic bradycardia secondary to necessary drugs for dysrhythmia management
- Symptomatic bradycardia resulting from 2nd degree AV block
- Chronic bifascicular or trifascicular block with intermittent 3rd degree or 2nd degree AV block
- Exertional 2nd or 3rd degree AV block
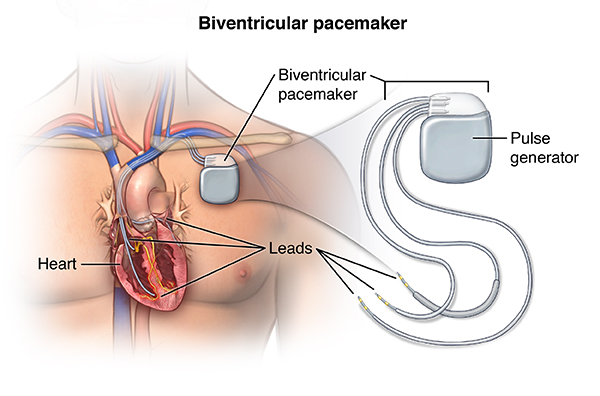
Biventricular Pacing (spectrumhealth.com)
Pacemaker Components
- Pulse Generator
- Houses power source (almost always lithium battery)
- Battery duration: 4-10 years (depends on features of device)
- Power decreases gradually with lithium battery; no abrupt cessation of activity
- Electronic Circuitry
- Leads
- Single lead: endocardial lead positioned in contact with right ventricle
- Dual lead: endocardial lead positioned in contact with right atrium and right ventricle
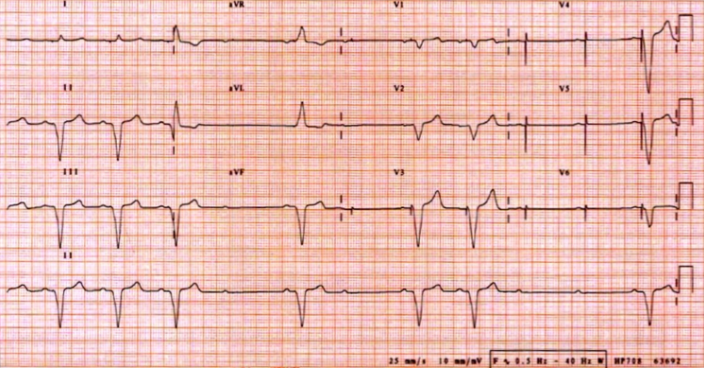
Sample Normal EKGs
- EKG appearance depends on type of pacemaker in use
- Single Ventricular Lead
- Narrow “spike” represents pacemaker generated electrical stimulus
- Followed by LBBB formation QRS complex
- Note: RBBB formation signifies lead displacement
- Dual Chamber Pacing
- Two narrow “spikes” seen representing an atrial stimulus (1st spike) and ventricular stimulus (2nd spike)
- First spike results in atrial depolarization. Second spike results in ventricular depolarization
- Ventricular response variable
- Narrow QRS
- Conducted from intrinsic atrial activity
- Conducted from pacemaker generated atrial spike via the AV node
- Atrial spike conducted through AV node and generates QRS
- Wide QRS
- Generated by ventricular lead stimulus
- Narrow QRS
- Absence of paced complexes in a patient with a pacemaker does not always indicate pacemaker dysfunction. It may reflect adequate native conduction and, thus, inhibition of the pacemaker
Normal Functioning Pacemaker EKGs

Atrial Paced Rhythm (LITFL)

AV Sequential Pacing (LITFL)

Ventricular Paced Rhythm (LITFL)

Ventricular Paced Rhythm II (LITFL)

Pacemaker Pocket Infection (researchgate.com)
Complications
- Infectious Complications
- Rare
- Pocket infection: 2%
- Bacteremia: 1%
- Signs/Symptoms: warmth, swelling, erythema, pain, fever
- Blood cultures: (+) in 20-25% of patients (commonly S. Aureus, S. epidermidis)
- Can result in pacemaker pocket erosion
- Treatment
- IV antibiotics (i.e.vancomycin)
- Needle aspiration: should only be performed under fluoroscopy to avoid cutting components of the device
- Cardiology consultation for removal and replacement
- Rare
- Thrombophlebitis
- Common complication (30-50% with some venous obstruction) (Kucher 2011)
- Symptoms
- Occur in only 0.5 -3.5% of patients due to collateralization
- Pain, swelling, venous engorgement of the ipsilateral arm
- Diagnostic Testing: Duplex sonography
- Treatment: Anticoagulation
- Pacemaker Syndrome
- Definition
- Loss of AV synchrony and loss of atrial “kick”
- Occurs when there is intact sinus node function but atria contract with tricuspid/mitral valves closed (i.e. during ventricular systole)
- Symptoms: Syncope/Near-syncope, orthostatic dizziness, exercise intolerance, generalized weakness, palpitations
- Treatment: replacement of single chamber pacemaker to dual chamber pacemaker
- Definition
Pacemaker Manufacturer
- In order to interrogate a pacemaker, the device manufacturer must be known
- The majority of the time, this information can be determined from the medical record or, the patient will carry a device manufacturer card with all of the information
- Algorithm to determine manufacturer using X-ray (Jacob 2011)
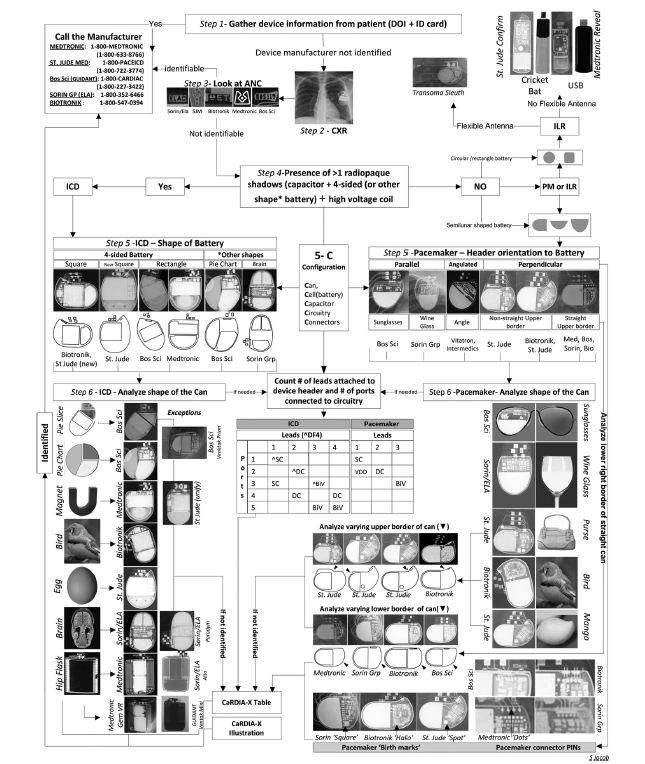
CaRDIA-X Algorithm
Effect of Magnet on Pacemaker (Core EM Video Link)
- Magnet application over a pacemaker will lead the pacemaker to default to the “magnet mode”
- Typically will lead to asynchronous pacing mode (does not turn off the pacemaker)
- Results in a constant paced rate regardless of the native rate or rhythm (eliminates sensing function)
- Either AOO, VOO or DOO
- The pacemaker will pace either the atrium, ventricle or both but will not sense or have a response to sensing
- Risk: Asynchronous ventricular pacing can lead to pacemaker-induced ventricular tachycardia
Pacemaker Malfunction
- Problems with Sensing
- Undersensing
- Definition: Pacemaker fails to sense native cardiac activity resulting in asynchronous pacing
- Can be complete or intermittent
- Commonly results from exit block
- Exit block: Failure of an adequate pacemaker stimulus to depolarize the chamber. Endocardium in contact with pacing lead requires higher stimulation threshold for conduction
- Exit block results from changes in cardiac tissue over time (i.e. an RV Infarction, progressive cardiomyopathy)
- EKG Findings
- Pacing spikes occurring earlier than the programmed rate
- Spike may not be followed by QRS complex if within the refractory period
- Presence of spikes within QRS complexes also suggestive (asynchrony)
- Oversensing
- Definition: Pacemaker mistakes electrical signals as native cardiac activity and thus, pacemaker function is inhibited
- Sources: Large P or T wave, pectoralis muscle contraction, cell phone signal (typically when on ipsilateral ear)
- Undersensing
- Problems with Pacing
- Output Failure
- Definition: No paced stimulus is generated from the device resulting in decreased or absent pacemaker function
- Causes: Oversensing, Lead displacement, Fracture of pacing wires
- Failure to Capture
- Definition: Electrical stimulus does not result in depolarization of the myocardium (no QRS complex generated)
- Causes: Exit block, myocardial infarction, lead displacement, wire fracture, electrolyte abnormalities
- Output Failure
Failure to Capture (LITFL)
- Pacemaker Associated Dysrhythmias
- Sensor-induced tachycardia
- Pacemakers designed to respond to physiologic stress by increasing heart rate (i.e. during exercise, hypercapnia, tachypnea)
- Pacemaker reacts to stimuli not intended to increase heart rate (vibrations, electrocautery, muscle contractions) resulting in inappropriate rate (rate will not exceed pacemaker’s upper rate limit)
- Treatment: Application of a magnet will terminate the pacemaker’s oversensing and result in pre-set pacemaker rate
-
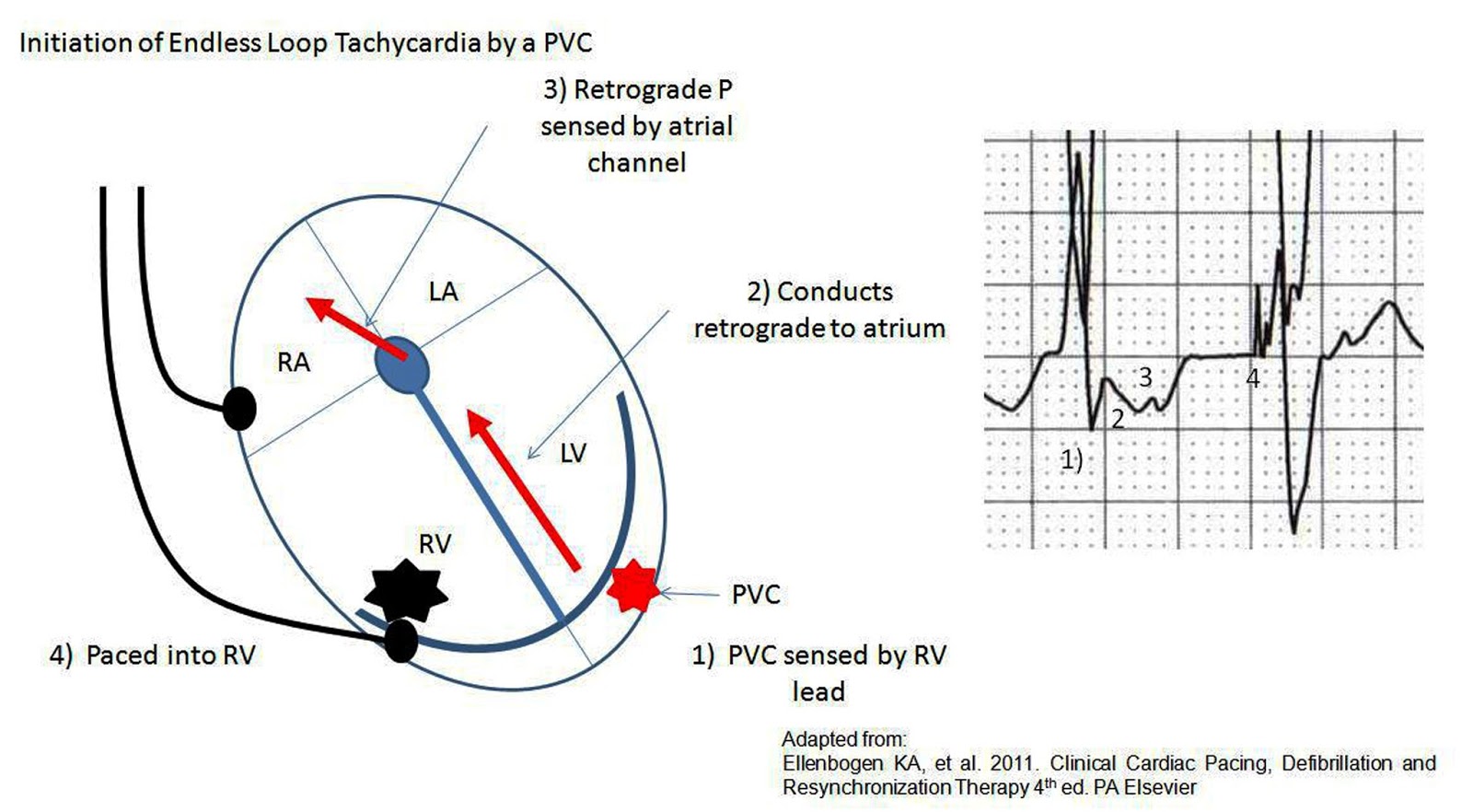
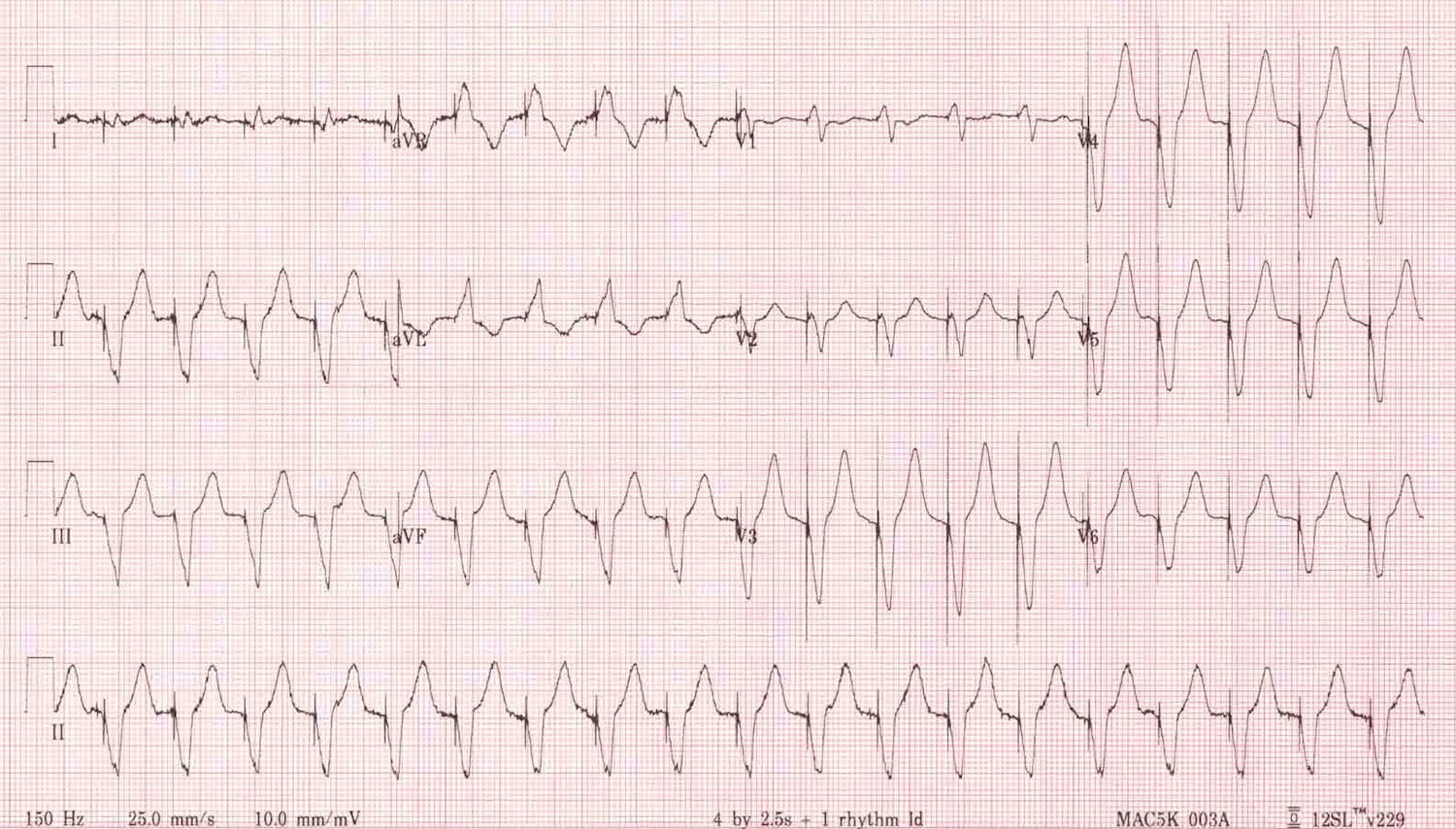
Pacemaker Mediated Tachycardia (learningecg.blogspot.com:)
Pacemaker mediated tachycardia (PMT) (aka endless loop tachycardia)
- Re-entry Tachycardia: Ventricular depolarization conducts retrograde into the atria leading atrial lead to detect activity as incoming P wave resulting in ventricular depolarization (viscous cycle develops)
- Treatment
- Administer AV blocker (adenosine, beta blocker, calcium channel blocker)
- Apply magnet over pacemaker
- Sensor-induced tachycardia
Pacemaker Mediated Tachycardia (LITFL)
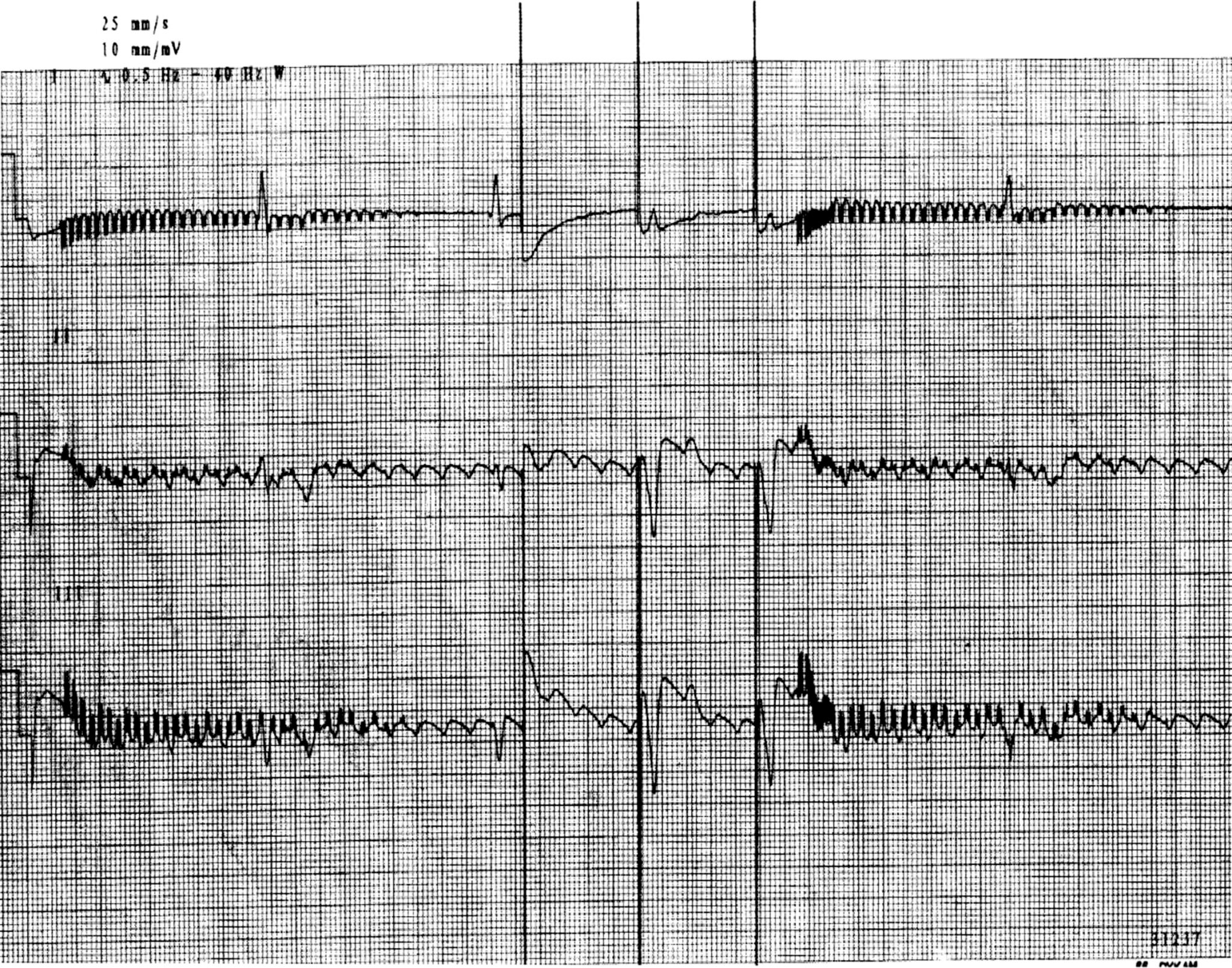
- Runaway pacemaker (Ortega 2005)
- Life-threatening malfunction seen in older-generation pacemakers resulting from low battery voltage
- Pacemaker delivers runs of pacing spikes in excess of 2000 bp
- Can provoke ventricular fibrillation
- Can also cause failure to capture as spikes low amplitude
- Treatment
- Apply magnet over pacemaker
- Replace pacemaker
Runaway Pacemaker (LITFL)
- Lead displacement dysrhythmia
- Results from a dislodged pacing wire “floating” around the right ventricle
- EKG: May demonstrate changing QRS morphology
- CXR: May aid in diagnosis
- Twiddler’s Syndrome
- Dysfunction of the pacemaker resulting from patient manipulation of the pulse generator
- Repeated manipulation results in the pacemaker rotating on it’s axis and dislodgment of the pacing leads
- Can cause pacing of the diaphragm or brachial plexus (arm twitching)
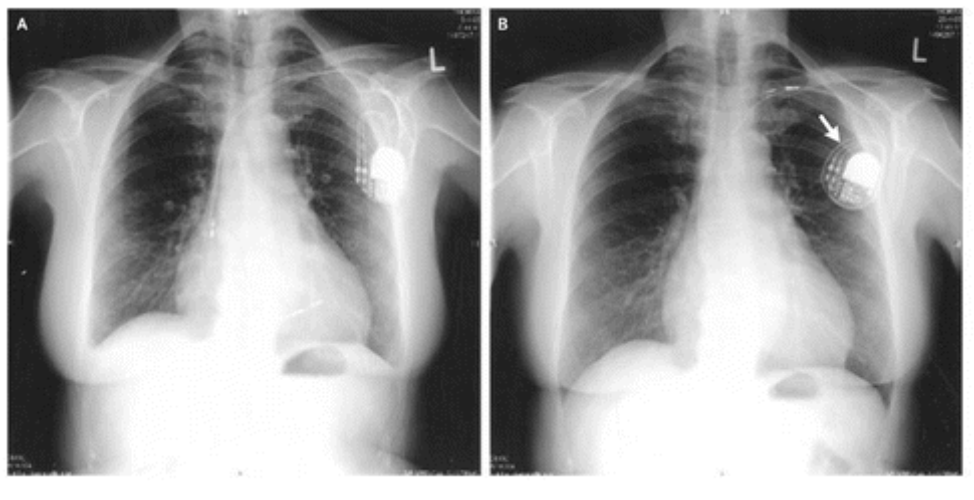
Twiddler’s Syndrome (NEJM)
Read More
LITFL: Pacemaker Rhythms – Normal Patterns
LITFL: Pacemaker Malfunction
Canadiem: Pacemaker Essentials: What We Need to Know in the ED
Core EM: How to Use a Magnet for Pacemakers + ICDs
Riemann JT, Squire B: Implantable Cardiac Devices, in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2010, (Ch) 80: p 1064-75.
References
Kucher N. Deep-vein thrombosis of the upper extremities. NEJM 2011; 364:861. PMID: 21366477
Jacob S et al. Cardiac rhtyhm device identification algorithm using X-Rays: CaRDIA-X. Heart Rhythm 2011; 8(6): 915-22. PMID: 21220049
Ortega DF. Runaway pacemaker: A forgotten phenomenon? Europace 2005; 7(6): 592-7. PMID: 16216762
