Anatomy of Orbital Fractures
- Orbit divided into 4 walls, made up of multiple bones (Tintinalli et al., 2016)
- Superior: Frontal
- Lateral: Zygoma and Sphenoid
- Inferior: Zygoma and Maxilla
- Medial: Ethmoid, including the lamina papyracea
- Inferior and Medial walls are the weakest and most commonly fractured
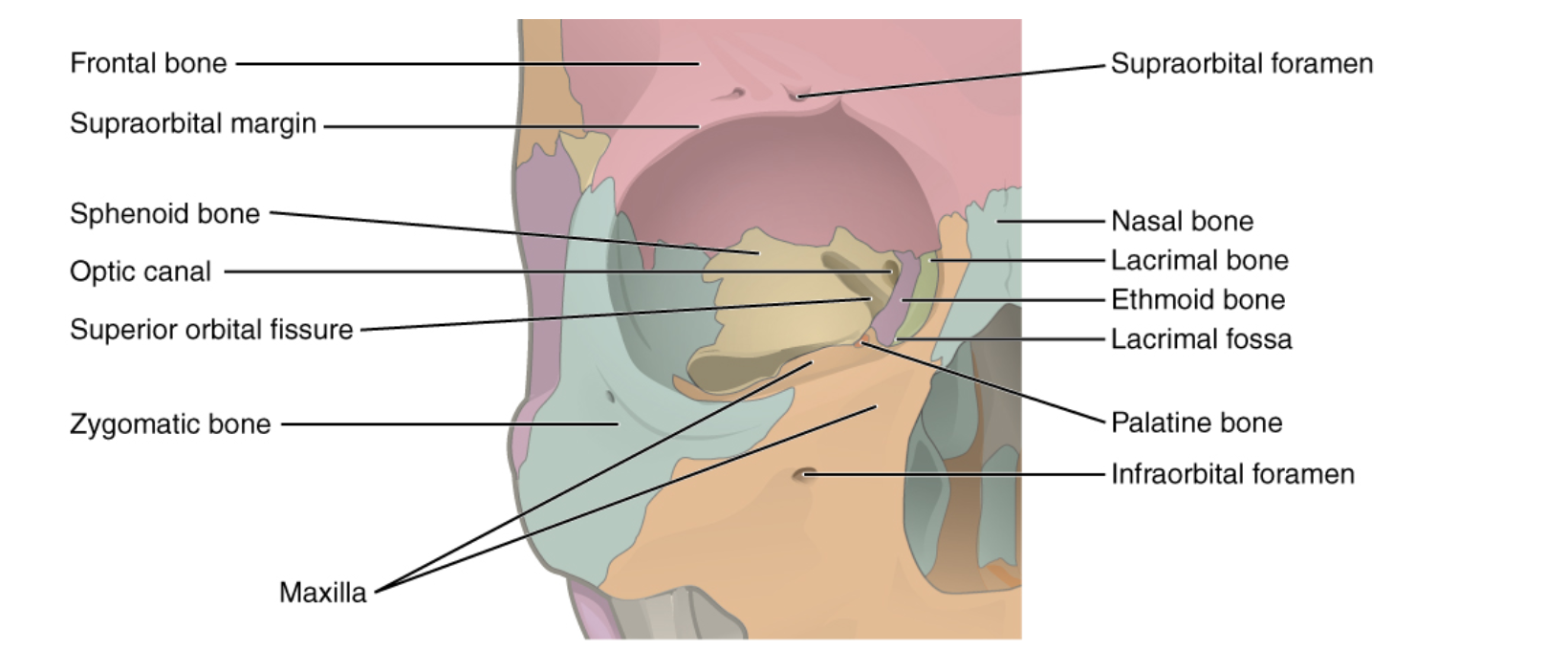
Orbit Anatomy (https://opentextbc.ca/anatomyandphysiology/chapter/7-1-the-skull/)
Orbital Blow-Out Fractures
- Any fracture of inferior or medial walls
- Force is transmitted through globe and results in fracture of the fragile inferior or medial orbital walls
- Pure Blow-Out Fracture
- Isolated fracture of orbital walls
- Occurs when small object strikes globe directly, without causing orbital ridge or rim fracture
- Associated with higher risk of ocular injury compared to Impure fractures
- Impure Blow-out Fracture
- Orbital rim is also injured
- Closed Door
- Non-displaced
- Trap Door (Fay & Dolman, 2017)
- Incomplete fracture of orbital bone
- More common in children due to soft bone
- Highest risk for entrapment
- Intraorbital contents herniate through fracture, then fracture returns to original position causing entrapment
- Pure Blow-Out Fracture
- Fractures of other portions of the orbit and fractures of the orbital ridge result from high energy impacts and are frequently associated with other fractures or injuries
- Significant force applied to the nasal bridge can result in naso-orbito-ethmoid fractures that are often accompanied by injury to the lacrimal duct, dural tears, and traumatic brain injury
Physical Exam
- Start with ABC’s
- Oculo-cardiac Reflex: Stretch receptors in ophthalmic nerve are activated in response to pressure in the ocular and periorbital soft tissue leading to stimulation of a vagal response (Dunville & Kramer, 2018)
- Results in bradycardia, nausea, and syncope; asystole is rare complication
- More common in children, but also in adults
- Patients with suspected retrobulbar hematoma should be monitored on telemetry until pressure is relieved
- Thorough eye exam is critical
- 1/3 of orbital wall fractures have concomitant ocular trauma (Kreidl, Kim, & Mansour, 2003)
- Every patient should have a complete eye exam including visual acuity, pupillary exam, slit lamp exam with fluorescein, ocular pressure testing
- Visual acuity is the most important measure of eye function
- Tear drop pupil should raise concern for globe rupture
- Enophthalmos – Early finding which precedes tissue edema
- Proptosis – Seen in retrobulbar hematoma
- Exam should also include:
- Extra-Ocular Eye Movements
- Diplopia on upward gaze is often seen in fractures of the inferior wall due to entrapment of inferior rectus, inferior oblique
- Palpation of orbital rim for step-offs
- Infraorbital anesthesia
- Due to injury to Maxillary Branch of Trigeminal Nerve (V2)
- Evaluation for crepitus
- Can be seen with medial wall fractures, particularly with nose blowing
- Extra-Ocular Eye Movements
Imaging
- Facial or Orbital Bone CT scan
- Gold standard imaging technique
- If there is high suspicion for orbital fracture based on exam, facial or orbital bone CT scan should be obtained as non-contrast head CT can miss a significant portion of facial fractures (Huang et al., 2017)
- Can see signs of eye emergencies such as globe rupture, retrobulbar hematoma, and entrapment in addition to the fracture itself
- Water’s View Skull X-Ray (Tintinalli et al., 2016)
- Prior to routine use of CT scans for patients with concern for facial trauma a Water’s view xray could be obtained to look for evidence of orbital fracture
- PA view of the skull with the head tilted back
- Look for fluid in the maxillary sinus and “Teardrop Sign”
- This view has become obsolete with the routine use of CT to diagnose orbital and other facial fractures
- Ultrasound
- Ultrasound should be avoided if there is any concern for globe rupture as manual pressure on the globe can precipitate further injury
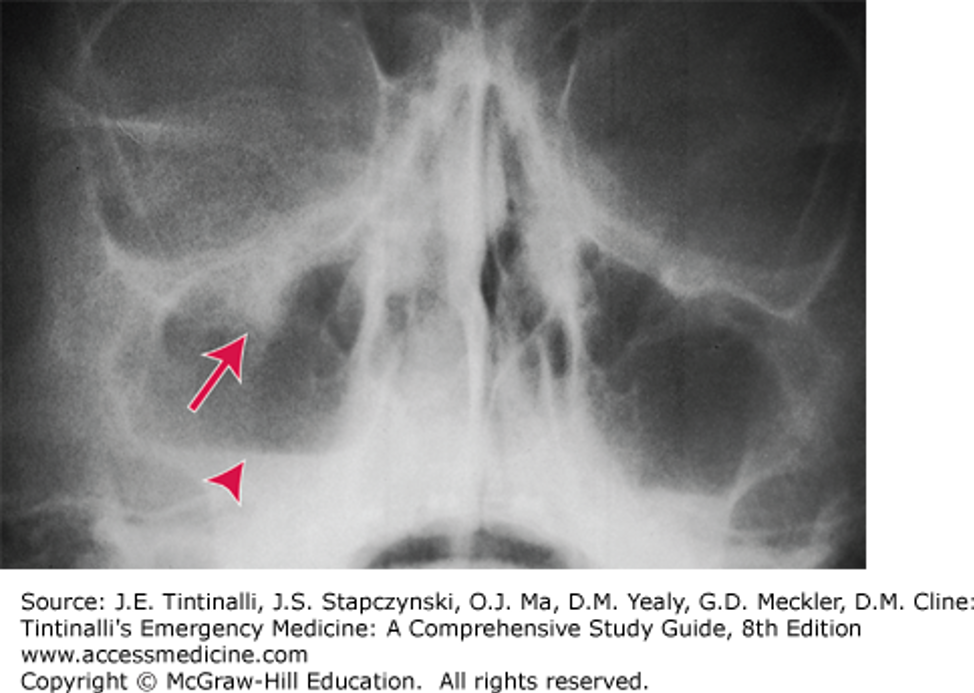
Water’s View Skull XR showing teardrop sign (arrow) and fluid in the maxillary sinus (triangle)

CT scan showing orbital blowout fracture (https://radiopaedia.org/cases/orbital-blowout-fracture-1?lang=us)
ED Management
- Main goal of ED management is to rule out associated orbital trauma, retrobulbar hematoma, and signs of entrapment
- Patients with globe injury, retrobulbar hematoma are ocular emergencies and should be evaluated by ophtho and facial trauma in the ED or transferred if specialty evaluation is unavailable
- Urgent (within 24hr) specialist evaluation should be obtained for patients with signs of entrapment or other non-emergent complications
- Patients with signs of entrapment may benefit from corticosteroids to reduce swelling
- Isolated orbital fractures without complications can be managed with:
- Oral antibiotics such as Augmentin
- There is poor evidence for routine use of antibiotics in orbital fractures, however they are routinely prescribed (Reiss et al., 2017)
- Nasal decongestant for 3 days
- Nose-blowing precautions
- Close (1-week) outpatient facial trauma and ophthalmology follow-up
- Oral antibiotics such as Augmentin
References
- Tintinalli J.E., Stapczynski J., Ma O., Yealy D.M., Meckler G.D., Cline D.M.. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e New York, NY: McGraw-Hill; 2016.
- Dunville LM, Kramer J (2018) Oculocardiac reflex. StatPearls Publishing, Florida, United States.
- Fay, A., & Dolman, P. J., editor. (2017). Diseases and disorders of the orbit and ocular adnexa.
- Huang, L. K., Wang, H. H., Tu, H. F., & Fu, C. Y. (2017). Simultaneous head and facial computed tomography scans for assessing facial fractures in patients with traumatic brain injury. Injury, 48(7), 1417-1422.
- Kreidl, K. O., Kim, D. Y., & Mansour, S. E. (2003). Prevalence of significant intraocular sequelae in blunt orbital trauma. The American journal of emergency medicine, 21(7), 525-528.
- Reiss, B., Rajjoub, L., Mansour, T., Chen, T., & Mumtaz, A. (2017). Antibiotic Prophylaxis in Orbital Fractures. The open ophthalmology journal, 11, 11-16.
Thank you for your lovely article from Johannesburg, South Africa.
In many Hospitals in South Africa, and most hospitals in Africa, CT scans are not readily available. Fortunately X-rays are. In this context a positive finding on a Water’s view is often the ticket for urgent up-referral, CT imaging and specialist consultation.
Thought I’d add my 2 cents on the matter.
Keep up the good work