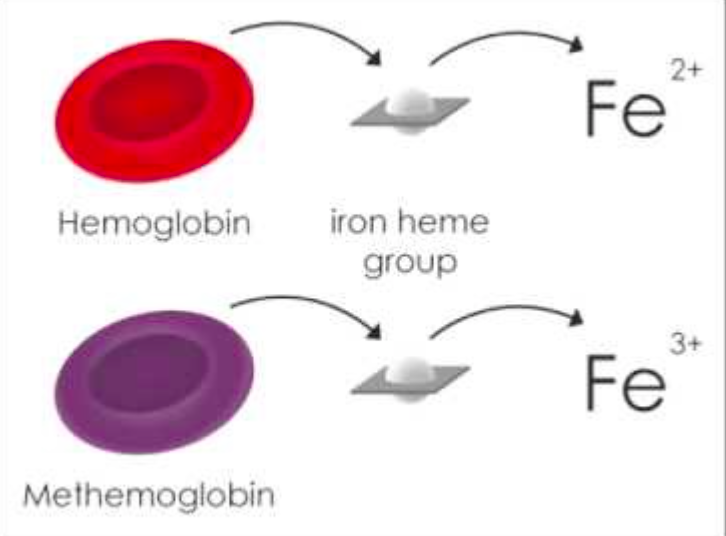
Definition: A hemoglobinopathy characterized by an abnormal elevation of methemoglobin (MetHb) – hemoglobin in which iron (ferrous Fe2+) has been oxidized(ferric Fe3+). An abnormal MetHb level is any level > 1%.
Methemoglobinemia Pathophysiology
Mechanism of Action
- Pathophysiology
- Oxidized iron sites on MetHb unable to bind oxygen
- Remaining binding sites with increased affinity for binding oxygen
- Causes a leftward shift in the oxyhemoglobin dissociation curve
- Results in decreased tissue oxygen delivery
- Normal situation
- Red cells constantly exposed to oxidant stress
- NADH MetHb reductase keeps oxidative stress in check by reducing MetHb to Fe2+ state
- Methemoglobinemia occurs when either
- There is an deficiency of the reducing enzyme (NADH MetHb reductase)
- There is increased oxidative stress that cannot be handled by the body
- Presence of MetHb renders pulse-oximetry readings inaccurate
Common Causative Agents
- Benzocaine
- Dapsone
- Nitroglycerin
- Nitrofurantoin
- Nitroprusside
- Phenazopyridine
- Sodium Nitrite
- Amyl nitrite
- Contaminated well water
- Isobutyl Nitrite (“poppers”)
Signs + Symptoms
- Low O2 saturation that does not respond to supplemental O2
- Key diagnostic feature (sat < 85% w/o response to 100% FiO2)
- Wavelength averaging by the pulse oximeter causes a falsely low O2 reading
- Since there is no true decrease in O2 saturation, there will be no response to 100% FiO2
- Severity of symptoms correlates closely to MetHb level and severity of impaired O2 delivery
- Symptoms will be worse for any MetHb level in patients with baseline impairment of O2 delivery (i.e. CHF, pneumonia, COPD, anemia)
-
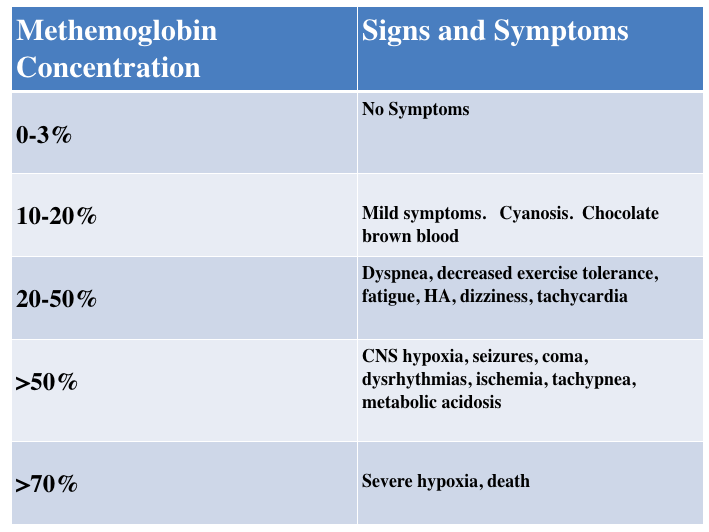
Methemoglobinemia Signs and Symptoms (Goldfrank’s Toxicology)
MetHb: < 15%
- May be asymptomatic
- Low pulse oximeter reading
- MetHb: 15-20%
- Cyanosis (peripheral and central)
- Fatigue
- Chocolate brown colored blood
- MetHb: 20-50%
- Dyspnea
- Headache
- Exercise intolerance
- Dizziness
- Syncope
- Weakness
- MetHb: 50-70%
- Tachypnea
- Metabolic acidosis
- Dysrhythmias
- Seizures
- CNS depression
- Coma
- MetHb > 70%
- Severe hypoxemia
- Death
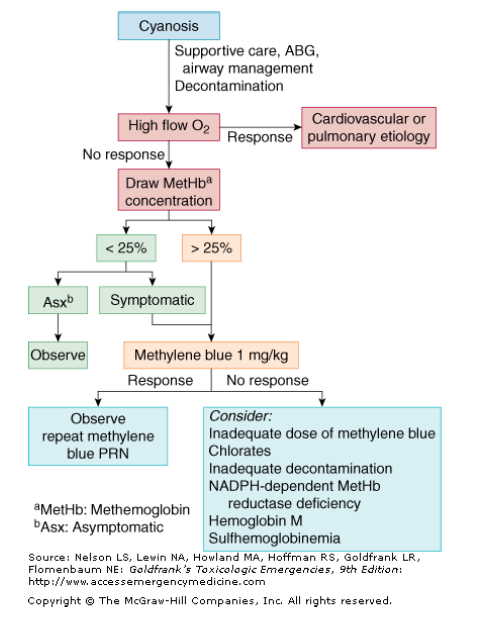
Toxicologic Assessment of Cyanosis (Goldfrank’s Toxicology)
Management
- Source identification, removal (if possible) and decontamination
- Basic Supportive Care
- Provide 100% FiO2 – lack of response should raise suspicion of methemoglobinemia
- Due to unreliability of pulse oximetry, O2 saturation should not be sole indication for advanced airway management
- Diagnostic Testing
- Blood gas
- Venous blood gas (VBG) adequate
- Arterial blood gas (AG) if obtained, will reveal a normal PaO2
- Co-oximeter panel for MetHb level
- Can use a venous or arterial sample
- Half-life 1-3 hours
- Blood gas
- Obtain toxicology consultation (800-222-1222 in US)
- Methylene Blue
- Mechanism of action
- Converted to cofactor for NADPH MetHb reductase
- Helps increase reduction of MetHb
- Which patients should get treatment?
- MetHb < 25% with symptoms
- Abnormal vital signs
- Metabolic acidosis
- End organ dysfunction (i.e. AMS, seizures)
- MetHb > 25% regardless of symptoms
- MetHb < 25% with symptoms
- Dosing
- 1-2 mg/kg IV
- Medication can cause local painful reaction
- Minimize with slower infusion (over 5 minutes)
- Flush line after infusion completed
- Clinical improvement should occur rapidly
- Warning: Will cause transient decrease in puse-ox level due to color of medication
- Mechanism of action
Take Home Points
- Methemoglobinemia can result from exposure to a number of different medications. The most common are dapsone and topical anesthetic agents (i.e. benzocaine)
- Consider the diagnosis in any patient with cyanosis and hypoxia that doesn’t respond to oxygen administration
- Administer methylene blue to any patient with abnormal vital signs, metabolic acidosis, end organ dysfunction or, a serum level > 25%
Read More
Core EM: Episode 97.0 – Methemoglobinemia
Price DP. Chapter 127. Methemoglobin Inducers. In: Nelson LS, Lewin NA, Howland M, Hoffman RS, Goldfrank LR, Flomenbaum NE. eds. Goldfrank’s Toxicologic Emergencies, 9e New York, NY: McGraw-Hill; 2011.. Link
