BACKGROUND
Definition
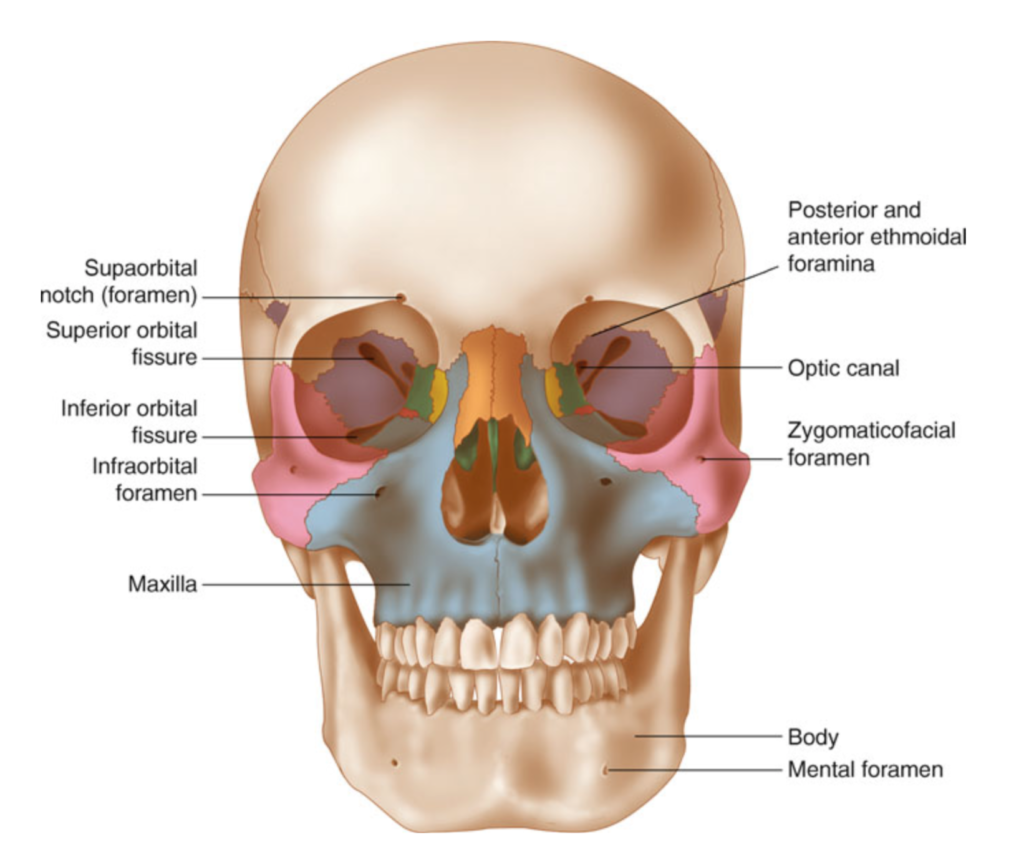
- Term applied to transverse fractures of the midface. The fractures involve three bones of the midface
- Maxilla
- Orbital rims
- Zygoma
- All involve the pterygoid processes of the sphenoid bones, which make up intrinsic support of the midface
- Results in discontinuity of the midface
 Hartstein 2012
Hartstein 2012
- Results in discontinuity of the midface
Fun fact: These fractures were named by Rene Le Fort, a French surgeon in 1901 who took intact cadavers and caused forceful blunt trauma to the skulls.
Epidemiology
- Low-velocity mechanism (fall from standing, blunt trauma) resulted in the majority of Le Fort I fractures (56%)
- High-velocity mechanism (fall >1 story, high-speed MVC) were associated with higher grade Le Fort fractures (e.g. II, III) (Phillips 2017)
- Associated head and neck injuries with higher grade Le Fort fractures: (ibid.)
- Skull fracture (40.7%)
- Closed head injury (5.4%)
- Cervical spine injury (5.4%)
Classification
Three types, dependent on the plane of injury
- Le Fort Type I: “Floating palate”
- Involves a transverse fracture through the maxilla. Occurs above the roots of the teeth and may result in mobility of the maxilla and hard palate from the midface
- Can be associated with malocclusion and dental fractures

- Le Fort Type II: “Floating maxilla”
- This fracture involves extension of the fracture superiorally. Includes fractures of the nasal bridge, maxilla, lacrimal bones, and orbital floors and rims
- Typically bilateral and triangular in shape

- Le Fort Type III: “Floating face”
- Rare but are considered “craniofacial dysjunction”
- They involve the bridge of the nose, the medial walls of the orbit (ethmoids), the lateral orbital walls, the maxilla and the zygomatic arch
- The entire face can shift

Phillips 2017
EVALUATION
Findings on presentation
- Severe facial ecchymosis (balloon face)
- Severe nasal or oral hemorrhaging
- Conjunctival hemorrhage.
- CSF Rhinorrhea
- Hemotympanum
- Anosmia
- Paresthesias of the face
- Elongation of the face
- Nasal disfiguration
- Emphysema of the face
- Exophthalmos
- Racoon eyes
- Auricular hematoma
- Pupil asymmetry
- Dental injuries
- Sinking over the anterior face (dish face)

Knoop, Atlast of Emergency Medicine, 3rd Ed.
Diagnostics
- Primary survey (ABCs) and then secondary survey (where your facial and ocular exam occur)
Physical exam
- Palpation of the entire face will detect most fractures
- Mobility in the hard palate (intraoral palpation) or maxilla when teeth are grasped and evaluated while stabilizing the forehead with the other hand
- Pertinent questions to ask if the patient is awake and alert:
- How is your vision? (document visual acuity)
- Does your bite feel normal?
- Does anything feel numb?
Imaging
- Dedicated facial CT
- Allows for imaging of orbits and fine fracture lines as well
- Consider CT C-spine given high incidence of concomitant cervical spine injury
- 1.4% of patients with concomitant c-spine fracture / dislocation (Hasler 2012)
- No role in plain films due to the complexity of the facial bones
MANAGEMENT
- Airway should always be managed first, protection from bleeding or mechanical disruption is key
- Severe bleeding may occur from the nose or oropharynx and these can be managed with anterior packing
- Posterior packing should be avoided if possible unless the skull base is known to be intact.
- In one series, 43.5% of patients with Le Fort III required tracheostomy (Bagheri 2005)
- After the primary stabilization is achieved, other management can occur
- Elevate the head of the bed to 40-60 degrees for anyone with a possible CSF leak (if not in spinal precautions)
- Administering IV antibiotics, especially if CSF leak known orsuspected (though this is not well supported by literature) (Soong 2014)
- First generation cephalosporins or Augmentin when sinus fractures are involved
- Perform secondary exam
- Disposition
- There is an association between Injury Severity Score (ISS) and grade of Le Fort fracture (Bagheri 2005)
- Majority of patient require admission; in one series:
- 52.2% placed in ICU
- 20.9% taken directly to OR (ibid.)
- Goal is to restore the facial skeleton and proper masticatory function
- Consult oral maxillofacial surgery (or whoever may be on call for facial trauma at your institution)
- Consider neurosurgery consult if CSF leak noted
- These patients commonly do not need intervention though
- Consider ophthalmology consult within 24 hours depending on any ocular damage or involvement
TAKE HOME POINTS
- Usually due to high velocity accidents, with an association b/w ISS and Le Fort grade
- These injuries tend to have low mortality, but the associated injuries with it usually do
- CT is the most specific and sensitive test for Le Fort fracture diagnosis
- Protect the airway and control any hemorrhage
- It is important to stabilize any serious injuries to airway, spine, chest, abdomen and skull prior to definitive treatment of facial bones
- Admit, consult for operative repair, +/- antibiotics for definitive management
Read More
Facial Fracture Management Handbook: Iowa Head and Neck Protocols
Radiopaedia: LeFort Fracture Classification
AO Surgery Reference (great for clinical exam pearls): Midface Exam
References
Bagheri SC, Holmgren E, Kademani D, Hommer L, Bell RB, Potter BE, et al. Comparison of the severity of bilateral Le Fort injuries in isolated midface trauma. J Oral Maxillofac Surg. 2005;63(8):1123-9. PMID: 16094579
Hasler RM, Exadaktylos AK, Bouamra O, Benneker LM, Clancy M, Sieber R, et al. Epidemiology and predictors of cervical spine injury in adult major trauma patients: a multicenter cohort study. J Trauma Acute Care Surg. 2012;72(4):975-81. PMID: 22491614
Hartstein ME, Wulc AE, Holck DEE. Midfacial rejuvenation. New York: Springer; 2012. xvi, 252 p.
Kaul RP, Sagar S, Singhal M, Kumar A, Jaipuria J, Misra M. Burden of maxillofacial trauma at level 1 trauma center. Craniomaxillofac Trauma Reconstr. 2014;7(2):126-30. PMID:25071877
Marx JA, Rosen P. Rosen’s emergency medicine : concepts and clinical practice. 8th ed. Philadelphia, PA: Elsevier/Saunders; 2014.
Phillips BJ, Turco LM. Le Fort Fractures: A Collective Review. Bull Emerg Trauma. 2017;5(4):221-30. PMID: 29177168
Salonen EM, Koivikko MP, Koskinen SK. Multidetector computed tomography imaging of facial trauma in accidental falls from heights. Acta Radiol. 2007;48(4):449-55. PMID: 17453528
Soong PL, Schaller B, Zix J, Iizuka T, Mottini M, Lieger O. The role of postoperative prophylactic antibiotics in the treatment of facial fractures: a randomised, double-blind, placebo-controlled pilot clinical study. Part 3: Le Fort and zygomatic fractures in 94 patients. Br J Oral Maxillofac Surg. 2014;52(4):329-33. PMID: 24602602
Tintinalli JE, Stapczynski JS, Ma OJ, Cline D, Meckler GD, Yealy DM. Tintinalli’s emergency medicine : a comprehensive study guide. Eight edition. ed. New York: McGraw-Hill Education; 2016. xliii, 2128 pages p.
