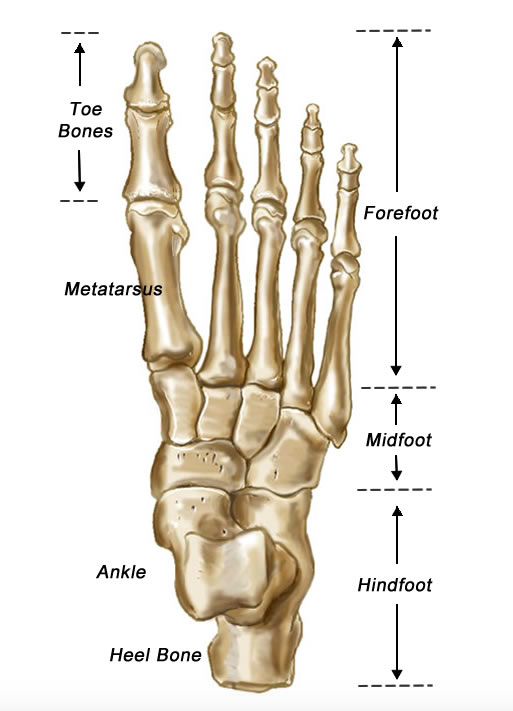
Foot Skeleton
Definition: Fracture of the base of the 5th metatarsal
- Proximal 5th metatarsal fractures are divided into 3 zones, each with their respective management and potential complications. (Dameron 1995)
Mechanism: Depends on the zone of injury
- Zone 1: Inversion injury
- Zone 2: Forefoot adduction
- Zone 3: Repetitive microtrauma (stress fracture)
Epidemiology:
- 5th metatarsal fractures represent 68% of all metatarsal fractures (Bowes 2016)
- Zone 1 is the most common proximal 5th metatarsal fracture (73%) with Zone 2 a distant 2nd (~20%) (Kane 2015)
Physical Exam
- Pain, swelling, and ecchymosis over lateral border of forefoot
- Point tenderness to palpation over the base of the 5th metatarsal
- Pain with weight bearing or inability to bear weight
- Ottawa Foot and Ankle Rules
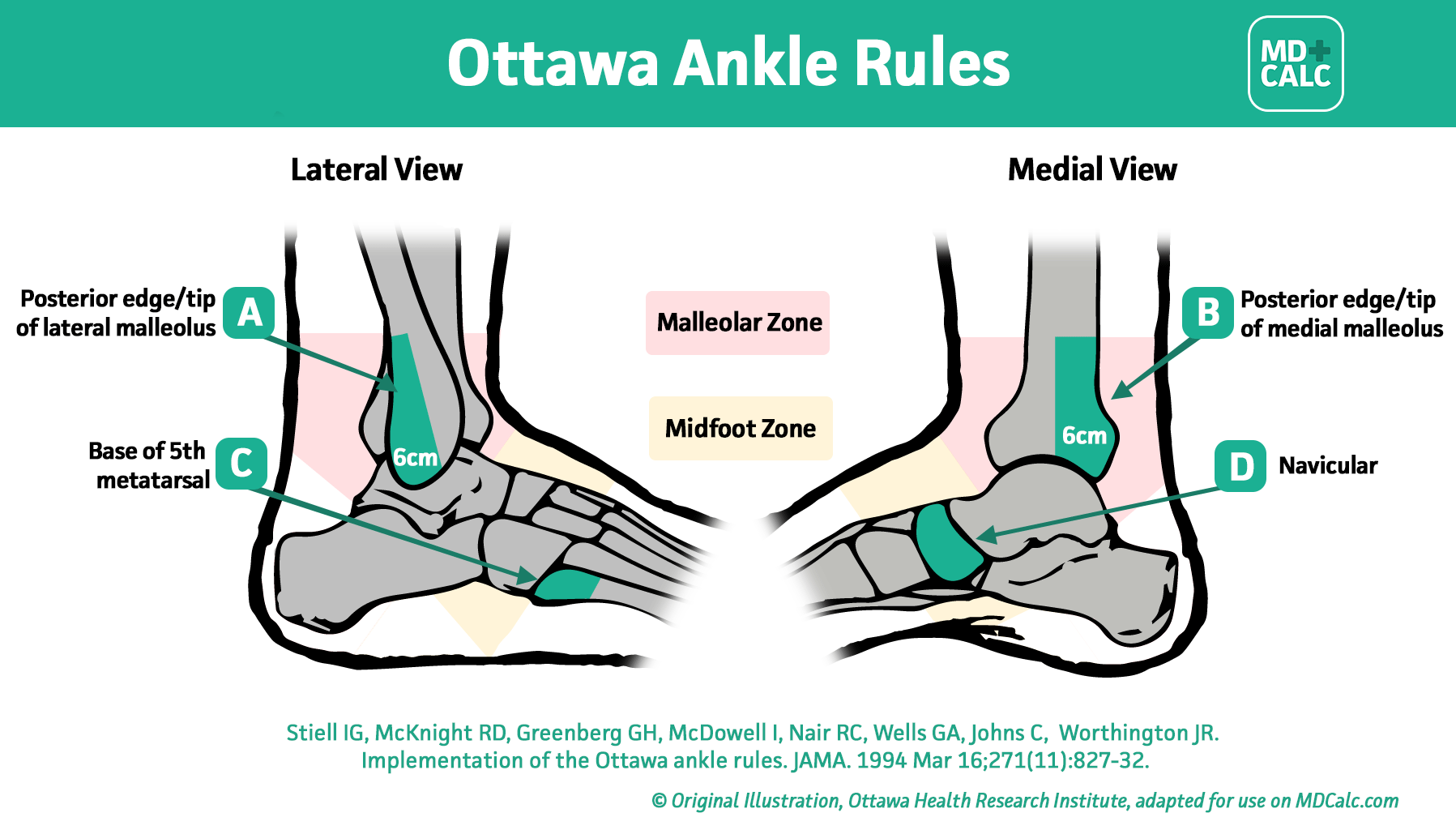
Ottawa Ankle Rules (MDCalc.com)
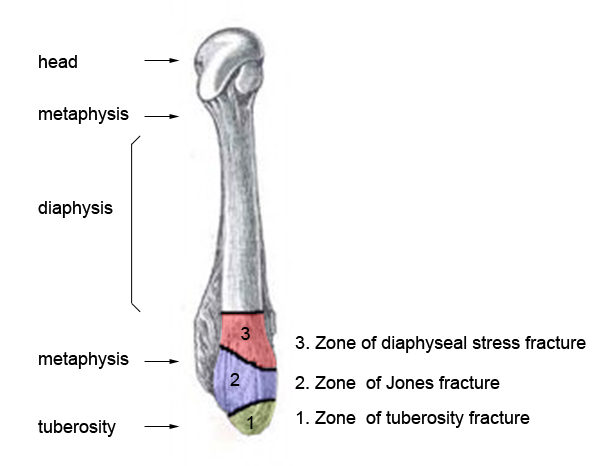
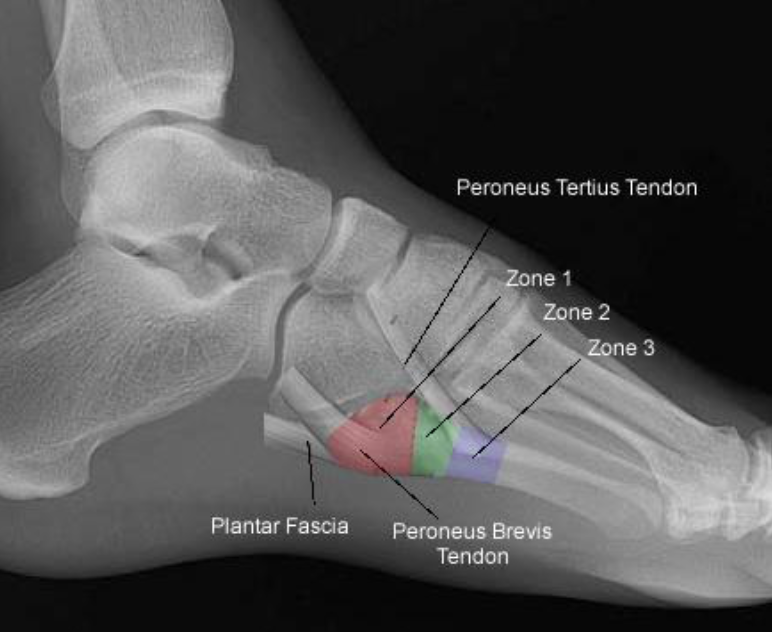
Zones of the 5th Metatarsal (wikifoundry.com)
Fracture Classification System
- Zone 1: Avulsion or “Pseudo-Jones” fracture
- Proximal tubercle (rarely enters 5th tarsometatarsal joint)
- Caused when bony fragment is detached by ligament or other connective tissue
- Typically long plantar ligament, lateral band of plantar fascia, or contraction of peroneus brevis
- Zone 2: Jones fracture
- Metaphyseal-diaphyseal junction (4th-5th metatarsal articulation)
- Vascular watershed area
- Proximal 5th metatarsal has unique blood supply with a watershed area at the metaphyseal-diaphyseal junction
- Fractures in this area are at a high risk for non-union due to the fracture interrupting the already limited blood supply in this area
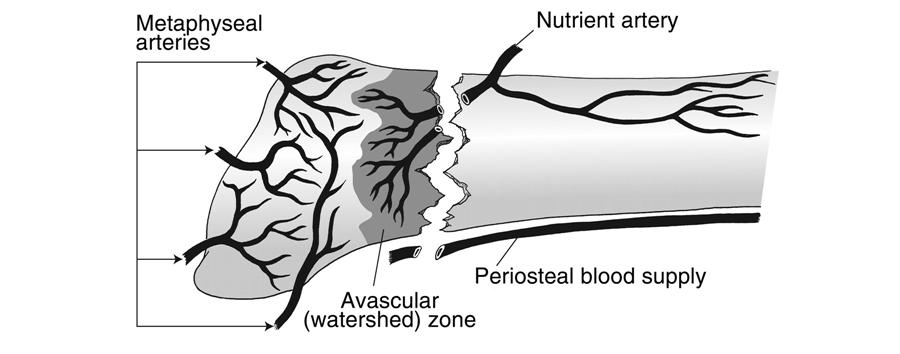
Vascular Watershed Zone (orthobullets.com)
- Zone 3: stress fracture
- Proximal diaphyseal fracture (distal to 4th-5th metatarsal articulation)
- Associated with cavovarus foot deformities or sensory neuropathies
5th Metatarsal Base Fractures (orthobullets.com)
Diagnostic Imaging
- Standard views of foot: AP, lateral, oblique
- Zone 1: fracture line extends into metatarsocuboid joint
- Zone 2: fracture in the metadiaphyseal junction of the 5th metatarsal base in which the main fracture line extends into the 4th-5th metatarsal articulation
- Zone 3: proximal diaphyseal fracture – instead of well-defined fracture lines, stress injuries may have widened fracture lines with surrounding cortical thickening

Jones Fracture (Case courtesy of A.Prof Frank Gaillard, Radiopaedia.org. From the case rID: 7638)
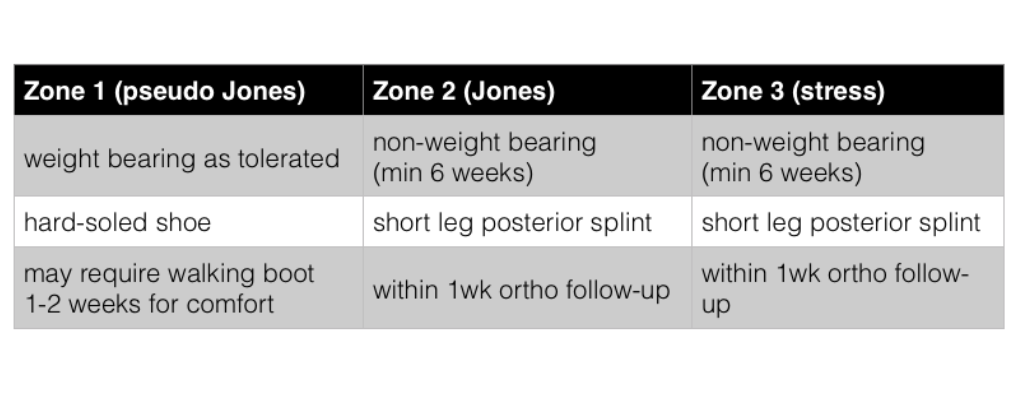
ED Management
- Analgesia
- Recommend elevation and icing for swelling
- Specific management by fracture location
Prognosis
- Zone 1: Heal very well, non-union is rare, can resume activities as tolerated
- Zone 2/3: Despite immobilization non-union can develop
- High-caliber athletes are frequently treated with intra-medullary screw fixation
- Non-union can lead to pain, difficulty ambulating, and possible need for surgery in the future
Take Home Points
- Location, location, location: Zone 1 (hard-soled shoe and WBAT) vs Zone 2/3 (splint and non-weight bearing) injuries require very different management
- Given similar mechanism, have high index of suspicion for 5th metatarsal fractures in typical ankle sprains
- Due to high risk of morbidity of missed Jones fracture, if you’re unsure, splint with strict non-weightbearing and err on the side of caution
Read More
Orthobullets: 5th Metatarsal Base Fracture
References
Bowes J, Buckley R. Fifth metatarsal fractures and current treatment. World J Orthop. 2016;7(12):793-800. PMID: 5155254
Dameron TB. Fractures of the Proximal Fifth Metatarsal: Selecting the Best Treatment Option. J Am Acad Orthop Surg. 1995;3(2):110–4. PMID: 10790659
Kane JM et al. The epidemiology of fifth metatarsal fracture. Foot Ankle Spec 2015; 8: 354–9. PMID: 25666689
Lutter LD, Mizel MS, Pfeffer GB, Orthopaedic Knowledge Update: Foot and Ankle. Rosemont IL: AAOS 1994
Petrisor BA, Ekrol I, Court-Brown C. The epidemiology of metatarsal fractures. Foot Ankle Int. 2006;27:172-174. PMID: 16539897
Thordarson DB. Orthopaedic Surgery Essentials: Foot & Ankle. Philadelphia, PA: Lipincott: 2004