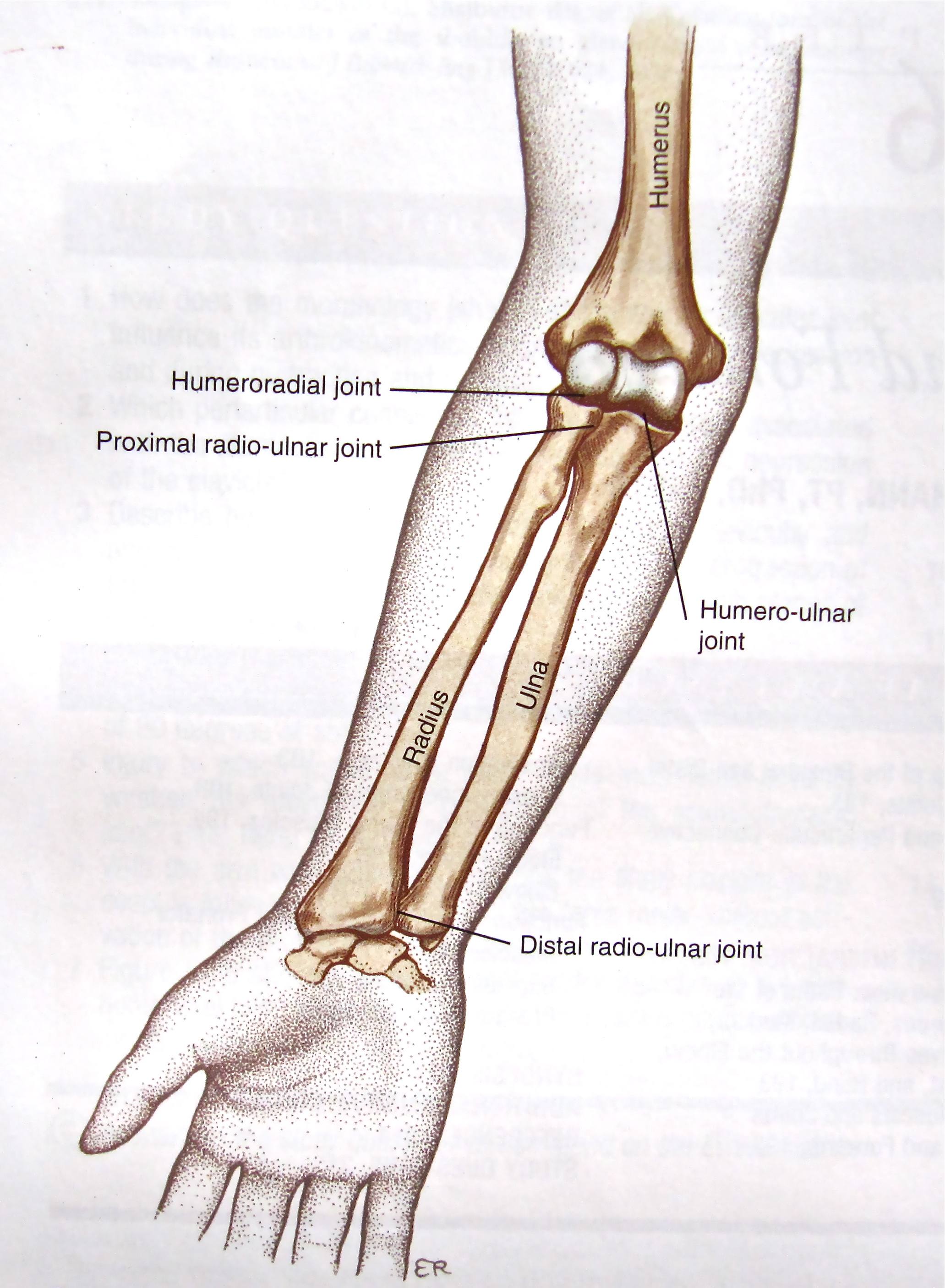
Bones of the Forearm (humananatomywiki101.com)
Definition
- Monteggia Fracture: Fracture of the ulnar shaft with associated radial head dislocation
- Galeazzi Fracture: Fracture of the radial shaft between middle and distal third with associated distal radial-ulnar joint (DRUJ) disruption
- Mnemonic: MUGR: Monteggia- Ulnar fracture, Galeazzi- Radius fracture
Mechanism
- Monteggia
- Fall onto outstretched and hyper-pronated hand
- Direct blow to ulna or hyperextension injuries
- Galeazzi
- Direct trauma to the wrist
- Fall onto outstretched and pronated hand
Epidemiology
- Adults: Estimated 60% of forearm fractures involve both bones, 25% fracture of only the ulna, 15% fracture of only the radius (Sonin 2000, Smith 1957)
- Exact incidence of Monteggia and Galeazzi fractures unknown
- Galeazzi estimated to account for 3-7% of forearm fractures
- Galeazzi fracture more common than Monteggia
- Monteggia more common in children, peak incidence 4-10 years old
Physical Exam
- Perform complete neurovascular exam in all patients concerning for either fracture
- Monteggia: Most common nerve injury posterior interosseous nerve (weakness with thumb extension)
- Galeazzi: neurovascular injury is rare
- Common to both fracture patterns are pain, elbow swelling, deformity, crepitus, painful and limited elbow ROM- especially pronation/supination
- Assess compartments for signs of increased compartment pressure
- ROM: assess for pain or limited ROM in supination and pronation as a sign of possible instability in both fractures
- DRUJ stress test: (for assessing for DRUJ instability in possible Galeazzi fractures)
X-Ray Findings
- Monteggia
- Ulna fracture is usually obvious. Avoid being distracted by this injury and missing the radial head dislocation
- Check radio-capetellar line
-
- Should intersect the capitellum regardless of angle of flexion/extension
- If it does not, indicates radial head dislocation
-

Radiocapetellar Line (Normal + Abnormal)

(http://www.wikiradiography.net/)
- Galeazzi
- Radius fracture usually obvious
- Check DRUJ
-
- The distal radioulnar joint is normally 1-2mm, wider suggests ligamentous injury
- Look for associated ulnar styloid fracture which can also suggest DRUJ injury
-

(http://www.wikiradiography.net/)
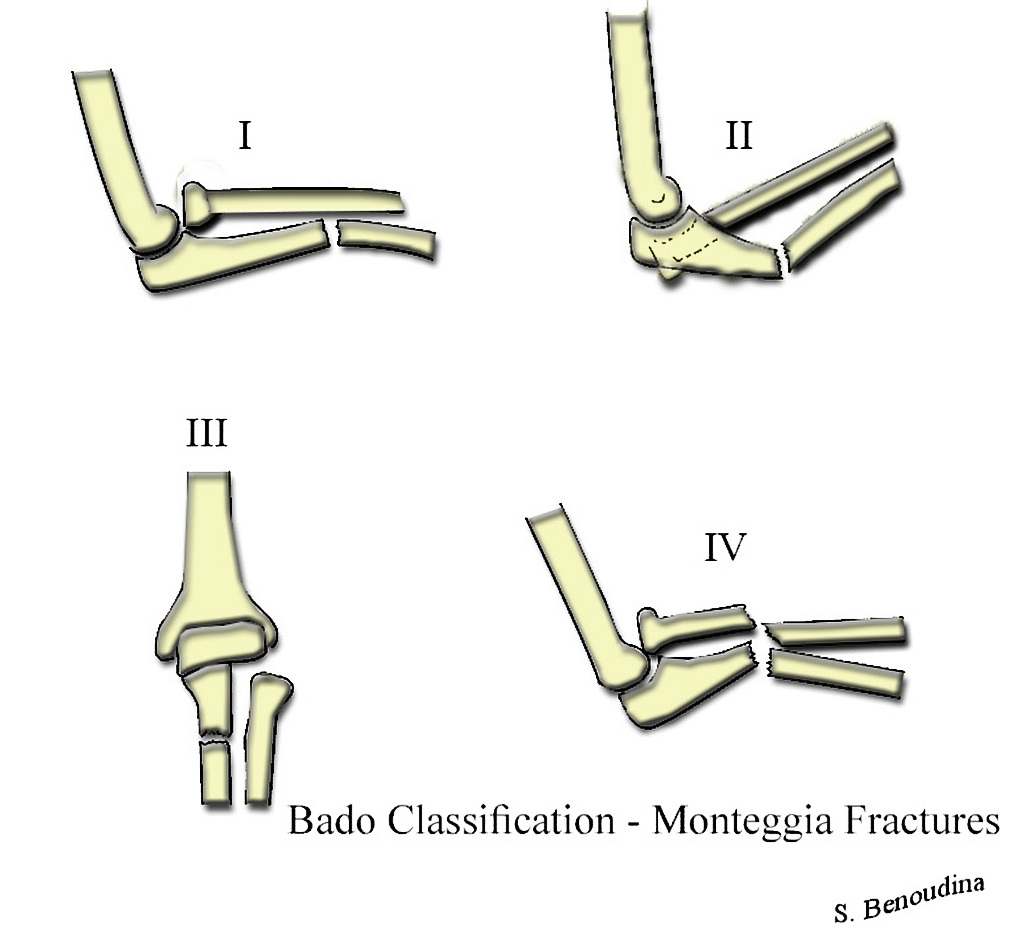
Bado Classification for Monteggia Fractures (Case courtesy of Dr Benoudina Samir, Radiopaedia.org. From the case rID: 39720)
Fracture Classification System
- Monteggia: Bado classification based on displacement of radial head
- Type I: Ulnar shaft fracture with anterior dislocation radial head
- Type II: Ulnar shaft fracture with posterior/posterolateral dislocation radial head
- Type III: Ulnar shaft fracture with lateral/anterolateral dislocation radial head
- Type IV: Ulnar shaft fracture with proximal shaft radial fracture at same level
- Galeazzi:
- Type I: Apex volar (dorsal displacement of distal radius)
- Type II: Apex dorsal (volar displacement of distal radius)
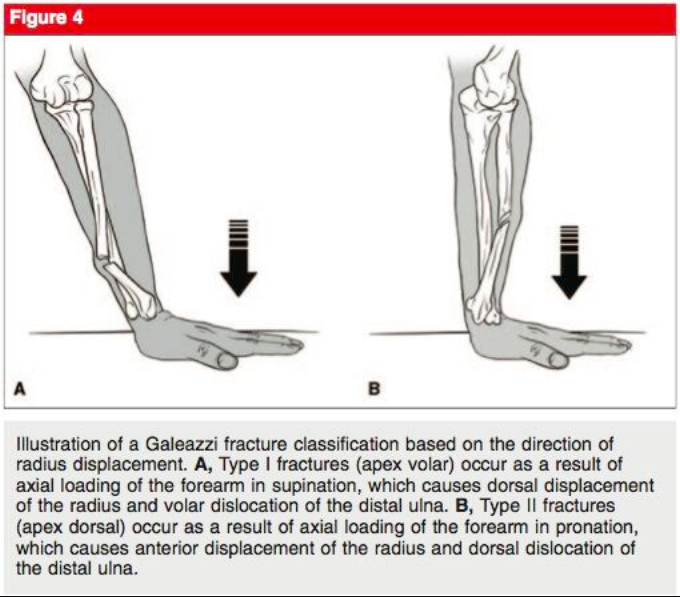
Galeazzi Type I + II Fractures (Atesok 2011)
ED Management
- General Care
- Provide analgesia
- Open fractures require immediate orthopedic consultation in the ED
- All cases should be discussed with an orthopedist
- If discharging from ED after reduction, all need close follow-up with orthopedics (within 1 week)
- Monteggia Fracture-Dislocations
- Pediatric Patients
- Priority is closed reduction of radial head, often made difficult by associated plastic/greenstick deformity
- Ensure anatomic alignment of the ulna and place in supinated long arm splint
- Inability to reduce radial head: Discuss with orthopedics for prompt consultation in ED vs admission for OR vs transfer to pediatric orthopedic referral center
- Usually managed conservatively if successful initial reduction.
- Adult Patients
- Priority is closed reduction of the radial head with attention to anatomic alignment of ulna with application of long arm splint
- If unable to reduce radial head, orthopedic consult in ED
- Managed with ORIF <1 week follow-up with orthopedics necessary
- Pediatric Patients
- Galeazzi Fractures
- Pediatric Patients
- Closed reduction of radius fracture and splinting with long arm splint in supination
- Managed conservatively, if non-reducible or unstable may require ORIF
- Adult Patients
- Closed reduction of the radius followed by reduction of the ulna in the DRUJ, with application of long arm splint
- If unable to reduce, orthopedic consult in ED
- “Fracture of necessity”
- Requires ORIF for acceptable outcome because of loss of stability at DRUJ and pull of forearm muscles causes loss of proper alignment in cast,
- High (up to 90%) complications rates seen if treated nonoperatively (Perron 2001, Hughston 1957)
- Pediatric Patients
Prognosis
- Misdiagnosis/ delayed diagnosis can lead to DRUJ instability, malunion, limited forearm ROM, chronic wrist pain, osteoarthritis, nerve injury
- Better long-term outcomes seen in children compared to adults
- Even with appropriate treatment, complications can include: PIN neuropathy (usually resolves), malunion, compartment syndrome, DRUJ subluxation
Take Home Points
- Always suspect a Monteggia/ Galeazzi injuries when a forearm fracture is seen as missed diagnosis can lead to very poor outcomes
- Radius Fracture: check for DRUJ injury
- Ulna Fracture: check for radial head dislocation
Read More
Ortho Bullets: Galeazzi Fractures
Ortho Bullets: Monteggia Fractures
Radiopaedia: Bado Classification of Monteggia Fracture-Dislocations
Core EM: Compartment Syndrome
References
Atesok KI et al. Galeazzi Fracture. J Am Acad Orthop Surg 2011; 19(10): 623-33. PMID: 21980027
Delpont M et al. Monteggia injuries. Orthop Traumatol Surg Res. 2017. PMID: 29174872
Egol KA et al. Handbook of Fractures 4th ed. Lipincott 2010: 261-268
George AV, Lawton JN. Management of complications of forearm fractures. Hand Clin. 2015; 31 (2): 217-33. PMID: 25934198
Hughston JC. Fracture of the distal radial shaft: mistakes in management. J Bone Joint Surg Am 1957; 39:249-264. PMID: 13416321
Johnson NP, Smolensky A. Fracture, Galeazzi. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2017 Jun-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470188/ PMID: 29262123
Perron AD et al. Orthopedic pitfalls in the ED: Galeazzi and Monteggia fracture-dislocation. Am J Emerg Med. 2001;19(3):225-8. PMID: 11326352
Smith H, Sage F P. Medullary fixation of forearm fractures. J Bone Joint Surg 1957; 39 91-98. PMID: 13385267
Sonin A. Fractures of the elbow and forearm. Semin Musculoskelet Radiol. 2000; 4(2): 171-91. PMID: 11061700
