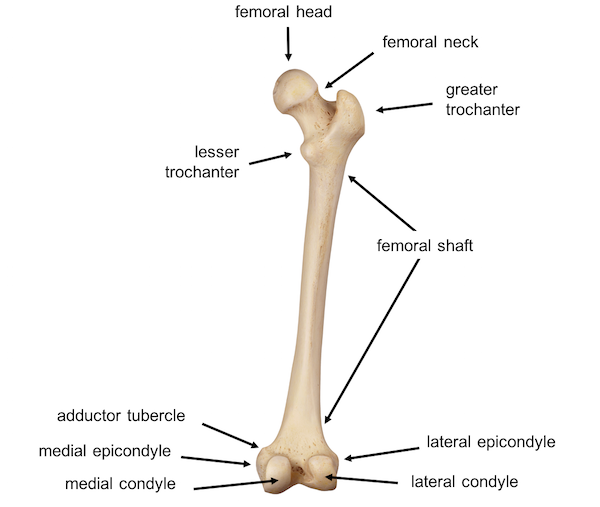
Femur Anatomy (anatomy.lexmedicus.com.au)
Definition: Fracture of the middle portion of the femur, which extends from the lesser trochanter to the femoral condyles.
Mechanism
- Younger population: High energy trauma such as MVA, fall from height, gunshots
- Older population: Low energy trauma such as fall from standing (Egol 2014)
Epidemiology
- Incidence of 37.1 per 100,000 person years in the U.S. (Arneson 1988)
- Most commonly occurs in males 15-24 and females 75 or older (Egol 2014)
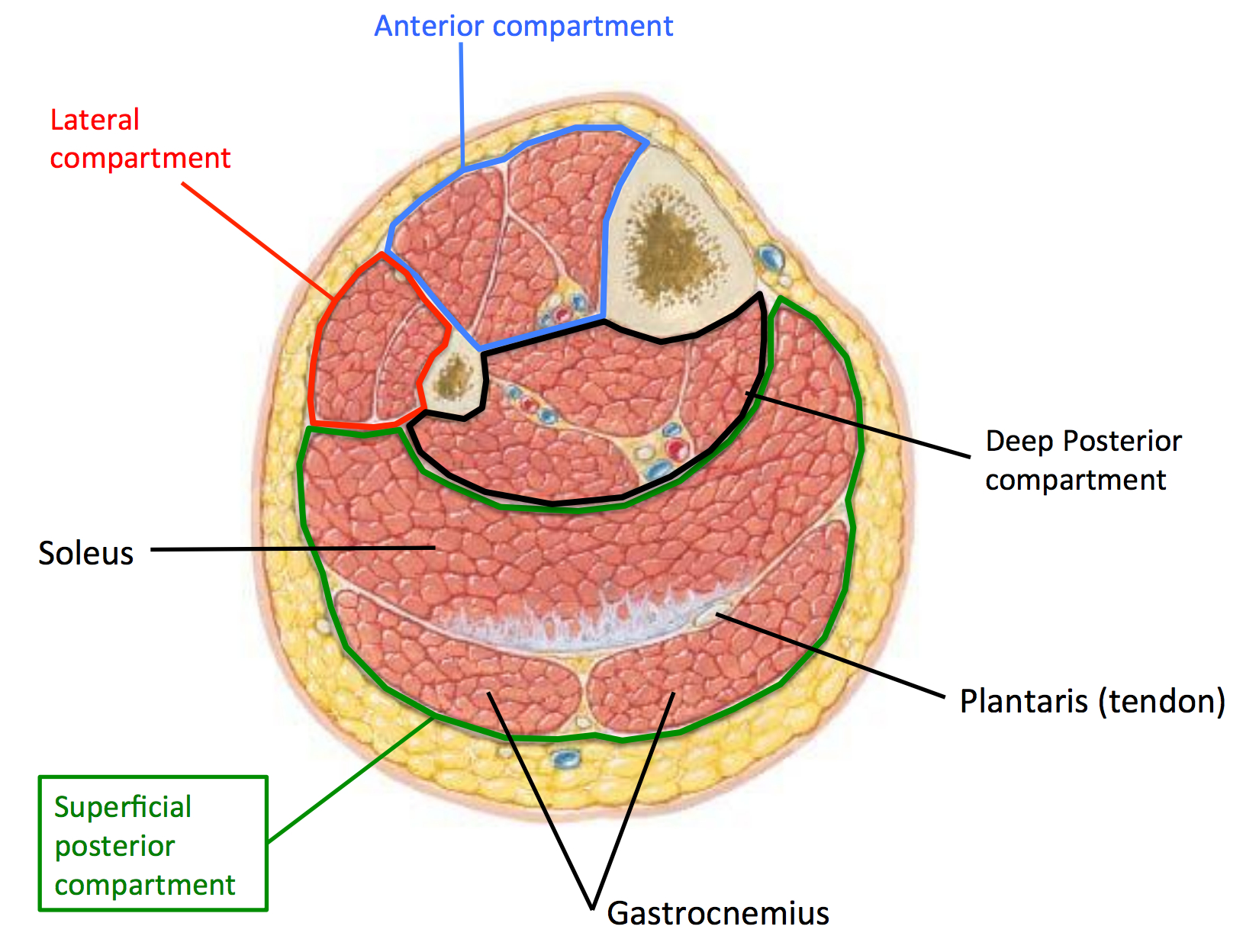
Cross Sectional View of Femur (anatomymedicalook.com)
Anatomy
- Muscles-Separated into three compartments
- Anterior Compartment (Sartorius, pectineus, quadriceps, illiopsoas), responsible for knee extension
Medial Compartment (gracilis and adductors longus, brevis, and magnus) - Posterior Compartment (biceps femoris semitendinosus, and semimembranosus), responsible for knee flexion
- Pull of these muscles in femoral fracture can result in angulation and displacement
- Neurovascular Supply
- Abundant supply primarily from profunda femoris artery
- Damage to sciatic/femoral nerve are rare due to protection by the muscles
Physical Exam
- Perform comprehensive trauma evaluation as there is a high association with other life threatening injuries
- Visual Inspection
- Presentation is not subtle. Typically will see a gross deformity
- Look for shortening of the extremity
- Palpation
- Tenderness to touch
- Assess compartment size for possibility of hemorrhage
- One of common locations for hemorrhagic shock to develop in trauma
- Average blood loss 1.2 liters but can be up to 3 liters (Lieurance 1992)
- Assess leg for signs of compartment syndrome
- Perform a complete neurovascular exam
- Associated injuries
- Pelvic/hip fracture and hip dislocations
- Femoral neck fractures occur in 1% to 9% of patients with femoral shaft fracture (Peljovich 1998)
- Ligament/meniscus injuries in 50% femur fx (Egol 2014)
Diagnostic Imaging
- Required views: AP Pelvis, AP Lateral Hip, Femur, Knee
- CT scan may be indicated to rule out other associated fractures, specifically femoral neck

Femoral Shaft Fracture II (wikipedia.com)
Ipsilateral Femoral Shaft and Neck Fracture (www.cjhr.org)

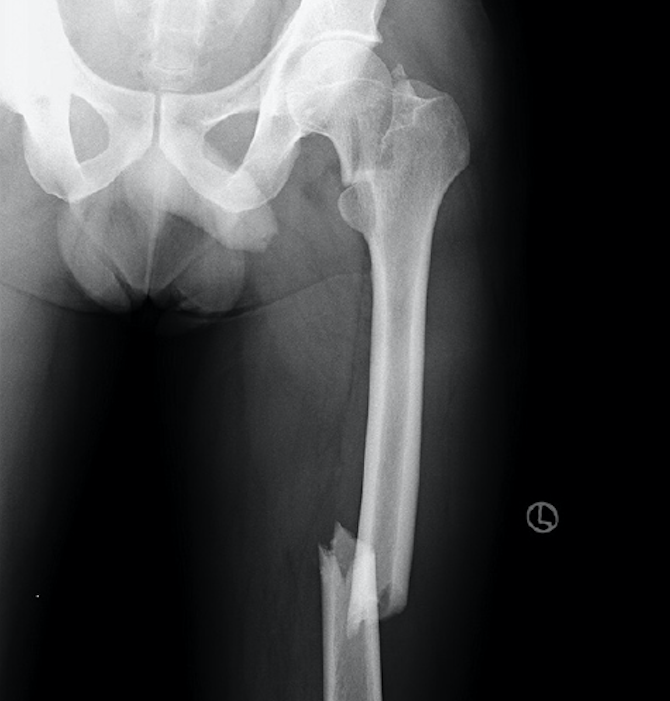
Segmental Femural Shaft Fracture (Case courtesy of Dr Benoudina Samir, Radiopaedia.org. From the case rID: 48182)
Fracture Classification Systems
Winquist and Hansen Classification
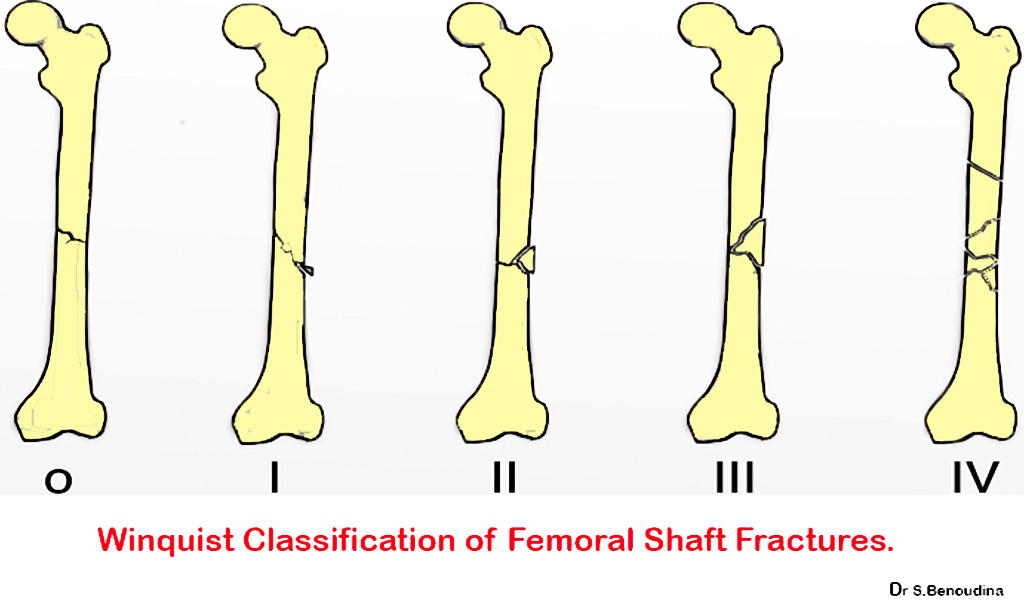
Winquest Classification of Femoral Shaft Fracture (Case courtesy of Dr Benoudina Samir, Radiopaedia.org. From the case rID: 48181)
OTA Classification System
OTA Classification of Femur Fractures (www2.aofoundation.org)
ED Management
- Orthopedic Consultation
- Pain control
- Intravenous opiates are often used as patients typically in severe pain
- Femoral nerve block (link)
- Highly effective for management of pain in femoral neck fractures
- Lower side effect profile than systemic analgesia
- Always calculate your toxic dose of local anesthetic to avoid local anesthetic systemic toxicity
- Closed fractures should be placed in long leg splint and can also be placed in traction
- Open Fractures should receive antibiotics and should proceed to OR for irrigation/debridement
- Skin Traction (Hare or Thomas)

Skin Traction Splint
Prognosis
- Antegrade reamed intramedullary nailing is associated with a 99% union rate and <1% rate of infection (Winquest 1984)
- With physical therapy young patients can return to baseline function in approximately 6 months (Paterno 2009)
- Older patients may take up to 1-2 years to have return to baseline function (Röder 2003)
- Complications include infection, malunion and non-union.
- Rare complications include neurovascular injury, hemorrhage, compartment syndrome, fat embolism, ARDS
Take Home Points
- Femoral shaft fractures are commonly associated with multi-system trauma.
- Do not get distracted by the obvious injury. Always remember to complete a thorough trauma evaluation
- Femoral nerve blocks are effective for pain management and have less side effects than systemic analgesics
- Placing the patient in a splint traction until your orthopedic colleagues arrive may improve alignment and improve blood flow
Read More
Orthobullets Femoral Shaft Fracture
Rosen’s Emergency Medicine Concepts and Clinical Practice(link)
Tintinalli’s Emergency Medicine(link)
References
Arneson TJ et al Epidemiology of diaphyseal and distal femoral fractures in Rochester, Minnesota, 1965-1984. Clin Orthop Relat Res 1988; 234: 188-94.PMID 3409576
Egol, KA, Koval, KJ, Zuckerman, JD. Handbook of Fractures. 4th ed. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins Health; 2014. link
Lieurance R et al Blood loss and transfusion in patients with isolated femur fractures. J Orthop Trauma. 1992;6(2):175. PMID:1602337
Nork SM. Fractures of the shaft of the femur. In: Rockwood and Green’s Fractures in Adults, 7th ed, Bucholz RW, Heckman JD, Court-Brown CM, et al (Eds), Lippincott, Williams & Wilkins, Philadelphia 2010. p.1656 link
Paterno MV et al Is there a standard rehabilitation protocol after femoral intramedullary nailing? J Orthop Trauma. 2009;23(5 Suppl):S39. PMID:19390375
Peljovich AE et al. Ipsilateral femoral neck and shaft fractures. J Am Acad Orthop Surg. 1998; 6(2):106-113. PMID:9682073
Röder F et al Proximal femur fracture in older patients–rehabilitation and clinical outcome. Age Ageing. 2003;32(1):74. PMID 12540352
Winquist RA et al Closed intramedullary nailing of femoral fractures. A report of five hundred and twenty cases. J Bone Joint Surg Am. 1984;66:529–539. PMID:6707031
The second picture shows the lower leg, not the thigh.
But nice website. I use it a lot.