BACKGROUND
- Prevalence of 2 to 4% with peak age of 18 to 24 months
- Seen from 6 months to 6 years
- Defined as a seizure with temperature >38 C without a central nervous system infection
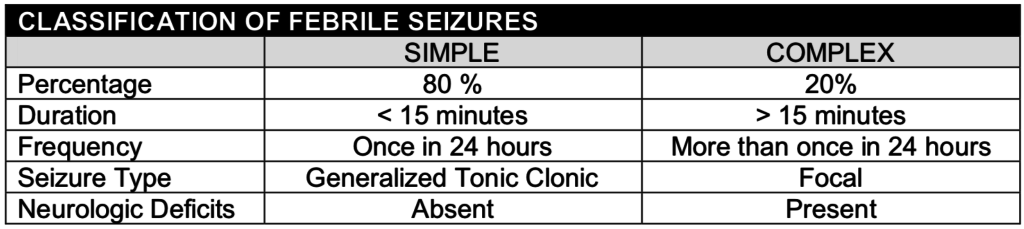
- Classified into two categories:
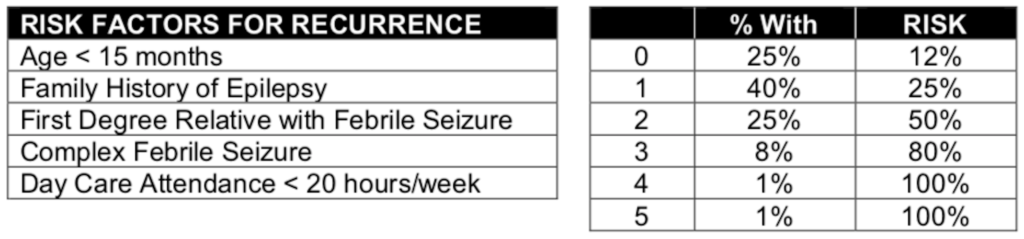
- Associated with increased risk: history of febrile seizures in a first or second degree relative, day care attendance, neonatal discharge greater than 28 days, and slow neurological development
- Any one of these factors increased the risk from 2 to 4% to 6 to 10%.
- 2 risk factors the incidence increases to 28% (Bethune 1993)
EVALUATION
- Clinical
- The diagnostic evaluation should be directed at establishing the cause of the fever rather than the seizure
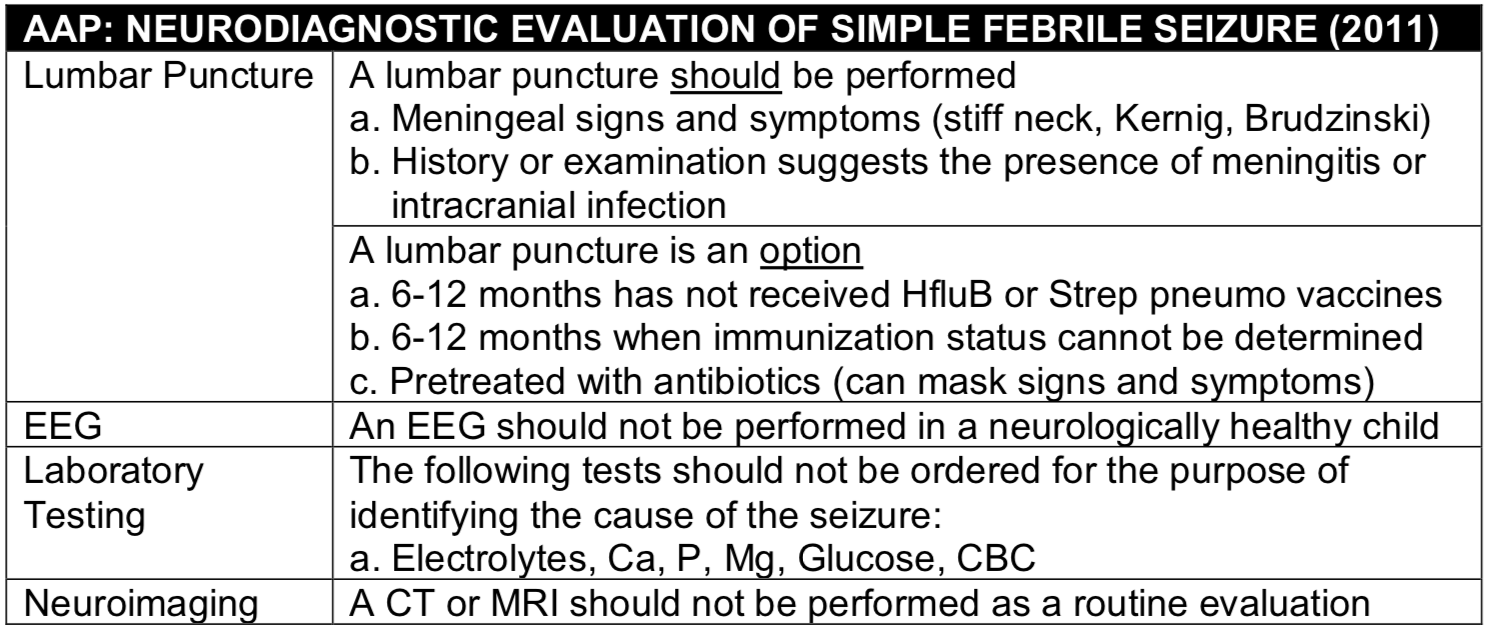
- A clinical practice guideline for neurodiagnostic evaluation of the child with a simple febrile seizure has been published by the American Academy of Pediatrics (AAP, 2011)
- Apply to neurologically healthy children 6 to 60 months presenting within 12 hours of a simple febrile seizure
- Laboratory
- Patients with a simple febrile seizure do not have an increased incidence of bacteremia or UTI
- Evaluation for a UTI, bacteremia or pneumonia should be based on the same criteria for patients with a fever but without a febrile seizure
- Lumbar Puncture
- A lumbar puncture should only be done if meningitis is suspected (e.g. no return to baseline after appropriate interval)
- In most studies, everyone with meningitis was clinically ill appearing or had obvious meningeal signs
- A study of 503 meningitis patients determined that 23% (115) had a seizure prior to diagnosis. 105/115 (91.3%) were obtunded or comatose. Of the remaining 10 patients, 8 had irritability and nuchal rigidity and 2 had complete febrile seizures. (Green 1993)
- In the past, it has been recommended that a lumbar puncture should be considered in patients with a complex febrile seizure
- A 2017 study included 2,839 patients presenting with a complex febrile seizure of which 31% had a lumbar puncture (Guedj 2017)
- Overall rate of bacterial meningitis was 0.7%
- Rate of bacterial meningitis in patients without an examination suggestive of meningitis was 0.0%
- Neuroimaging
- There is no role for a head CT or MRI in simple febrile seizures
- If the patient had a complex seizure, a head CT or MRI may be considered
- The incidence of a significant finding in this group is between 5 to 10%
- A 2017 study included 2,839 patients presenting with a complex febrile seizure of which 31% had a lumbar puncture (Guedj 2017)
MANAGEMENT
- Supportive care such as antipyretics for fever or antibiotics for an identified bacterial infection are generally the only treatment needed
- Antipyretics
- Many clinicians recommend the use of “around the clock” alternating antipyretics such as Acetaminophen or Ibuprofen
- In one study, Tylenol q6h at 10 mg/kg PR for the first 24 hours following the initial seizure was associated with a decreased rate of recurrence when compared to children who did not receive antipyretics (Murata, 2018)
- Antiepileptics
- Phenobarbital (Camfield 1980) and Sodium Valproate (Mamelle 1984) may decrease the incidence of future febrile seizures
- They are not routinely prescribed because of their long-term cognitive effects
- Rectal diazepam is sometimes prescribed for those with recurrent febrile seizures
- For patients with 2 or more risk factors for recurrence, giving rectal Diazepam at the onset of fever has been shown to decrease the risk of recurrence to 12% (Knudson 1985)
- Patients may present with an altered mental status due to the Diazepam making the evaluation of the need for a lumbar puncture difficult
DISPOSITION
- Simple febrile seizures can be safely discharged after the parents have been counseled
- Complex febrile seizures may require a more extensive evaluation and a neurology consult; admission should be considered in this group
PROGNOSIS
- Recurrence Risk
- The primary risk of simple febrile seizures is recurrence in approximately 1/3 of patients (14% at 6 months, 25% at 12 months and 30% at 24 months (Berg 1997)
-
- The lower the temperature that the patient has their febrile seizure at, the greater the chance or recurrence
- The incidence of recurrence if the febrile seizure occurs at 101 degrees is 35% and decreases in a linear fashion to 13% for a temperature of greater than 105 degrees (Berg 1992)
- There are data to support that the seizure occurs early on in the febrile event.
- There are no data to support the commonly held belief that a high rate of rise in temperature causes febrile seizures
- The lower the temperature that the patient has their febrile seizure at, the greater the chance or recurrence
- Epilepsy Risk
- The risk of epilepsy after a simple febrile seizure (1-2%) has been shown to be only slightly greater than the risk in the general population (0.5%)
- This risk increased in those with a family history of epilepsy, recurrence of febrile seizures and complex febrile seizures (Pavlidou 2013)
- The risk of epilepsy after a simple febrile seizure (1-2%) has been shown to be only slightly greater than the risk in the general population (0.5%)
- Cognitive Effects
- A febrile seizure has not been demonstrated to affect future intellectual ability (Verity 1998; Ellenberg 1978)
References
Berg AT, Shinnar S, Darefsky AS, Holford TR, Shapiro ED, Salomon ME, et al. Predictors of recurrent febrile seizures. A prospective cohort study. Arch Pediatr Adolesc Med. 1997;151(4):371-8. PMID: 9111436
Berg AT, Shinnar S, Hauser WA, Alemany M, Shapiro ED, Salomon ME, et al. A prospective study of recurrent febrile seizures. N Engl J Med. 1992;327(16):1122-7. PMID: 1528207
Bethune P, Gordon K, Dooley J, Camfield C, Camfield P. Which child will have a febrile seizure? Am J Dis Child. 1993;147(1):35-9. PMID: 7678187
Camfield PR, Camfield CS, Shapiro SH, Cummings C. The first febrile seizure–antipyretic instruction plus either phenobarbital or placebo to prevent recurrence. J Pediatr. 1980;97(1):16-21. PMID: 7381637
Ellenberg JH, Nelson KB. Febrile seizures and later intellectual performance. Arch Neurol. 1978;35(1):17-21. PMID: 619868
Green SM, Rothrock SG, Clem KJ, Zurcher RF, Mellick L. Can seizures be the sole manifestation of meningitis in febrile children? Pediatrics. 1993;92(4):527-34.PMID: 8414822
Guedj R, Chappuy H, Titomanlio L, De Pontual L, Biscardi S, Nissack-Obiketeki G, et al. Do All Children Who Present With a Complex Febrile Seizure Need a Lumbar Puncture? Ann Emerg Med. 2017;70(1):52-62 e6. PMID: 28259480
Knudsen FU, Paerregaard A, Andersen R, Andresen J. Long term outcome of prophylaxis for febrile convulsions. Arch Dis Child. 1996;74(1):13-8. PMID: 8660037
Mamelle N, Mamelle JC, Plasse JC, Revol M, Gilly R. Prevention of recurrent febrile convulsions–a randomized therapeutic assay: sodium valproate, phenobarbital and placebo. Neuropediatrics. 1984;15(1):37-42. PMID: 6424041
Murata S, Okasora K, Tanabe T, Ogino M, Yamazaki S, Oba C, et al. Acetaminophen and Febrile Seizure Recurrences During the Same Fever Episode. Pediatrics. 2018;142(5). PMID: 30297499
Pavlidou E, Panteliadis C. Prognostic factors for subsequent epilepsy in children with febrile seizures. Epilepsia. 2013;54(12):2101-7. PMID: 24304433
Subcommittee on Febrile S, American Academy of P. Neurodiagnostic evaluation of the child with a simple febrile seizure. Pediatrics. 2011;127(2):389-94. PMID: 21285335
Verity CM, Greenwood R, Golding J. Long-term intellectual and behavioral outcomes of children with febrile convulsions. N Engl J Med. 1998;338(24):1723-8. PMID: 9624192