Author:
- Sarah Beth Spiegel MD
Editor:
- Sarah Battistich, MD
- Jonathan Kobles, MD
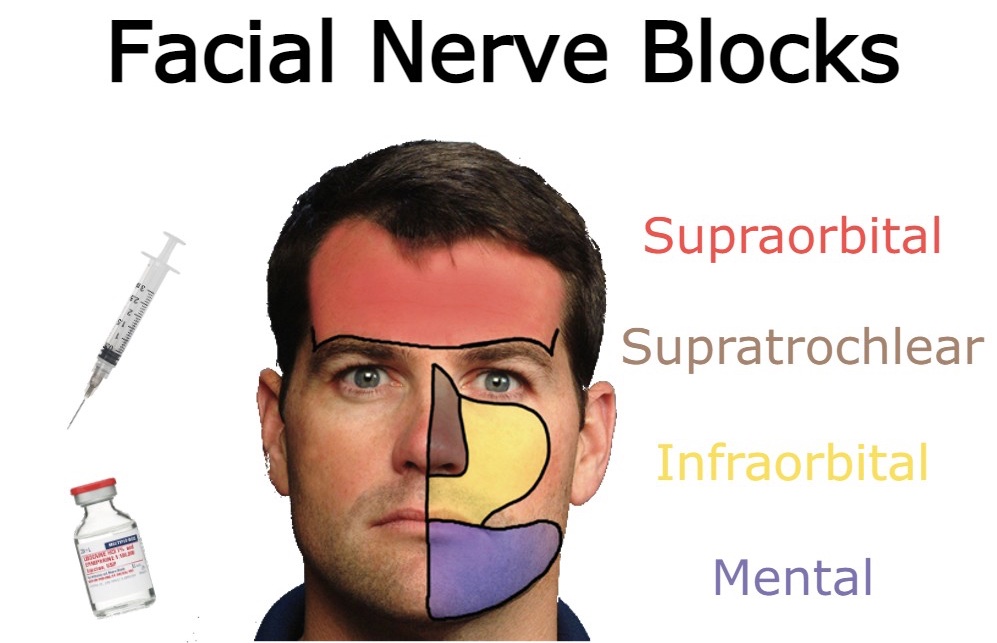
Facial nerve blocks offer an applicable option for achieving analgesia in the emergency department.
Potential Indications:
- Burn care
- Fractures and dislocations
- Large lacerations that would require a harmful dose of anesthetic
- Facial lacerations where distortion of the wound would affect the quality of repair
- Wound exploration
- Pain control (headaches, toothaches)
Contraindications:
- Infection around the injection site
- Bleeding disorders
- Preexisting nerve damage is a relative contraindication and should be well-documented before the procedure
Risks
- Nerve Injury
- Avoid intraneural injection and permanent nerve damage by advancing the needle slowly and monitoring for paresthesia. Parasthesia indicates that the needle tip is within the nerve sheath. Withdraw the needle 1-2mm, wait for the paresthesia to resolve, and then inject anesthetic.1
- Ultrasound guidance may also decrease the risk of intraneural injection.
Equipment:
- Chlorhexidine
- 18g draw up needle
- 20-27g injection needle
- Syringe
Commonly Used Anesthetics:
Lidocaine (1%) :
- Max dose: 3 mg/kg
- Duration: 30-120 mins
Lidocaine (1%) with epi :
- Max dose: 5 mg/kg
- Duration: 60-400 mins
Bupivacaine (0.25%) :
- Max dose: 1.75 mg/kg
- Duration: 120-240 mins
Bupivacaine (0.25%) with epi:
- Max dose: 2.25 mg/kg
- Duration: 240-480 mins
Tips and tricks for Pain Reduction:
- Consider the use of topical anesthetic (especially for pediatric patients )
- Use buffered anesthesia (3:1 ratio of 1% lidocaine to sodium bicarbonate)
- Warming anesthetic (allow to warm up by holding in pocket or hand)
Supraorbital Nerve Block:

Anatomy:
- The supraorbital nerve is a branch of the ophthalmic division of the trigeminal nerve.
- It emerges through the supraorbital foramen at the midline of the superior orbital ridge in line with the pupil.
- It is generally blocked together with the supratrochlear nerve.
Technique:
- Palpate the supraorbital notch.
- Insert the needle in the subcutaneous space superior to the eyebrow in line with the pupil.
- Direct the needle tip medially to create a horizontal wheel extending from the medial border of the brow using 2-5cc of anesthetic.
Infraorbital Nerve Block

Anatomy:
- The infraorbital nerve is a branch of the maxillary division of the trigeminal nerve. It runs out of the infraorbital foramen ~1cm inferior to the mid-infraorbital ridge and in line with the pupil.
- It provides sensory innervation to the medial cheek and upper lip.
- The infraorbital nerve branches into the anterior and middle superior alveolar nerves, providing sensation to maxillary incisors, canine, and premolar teeth.
Extraoral Technique:
- Palpate the infraorbital foramen.
- Insert needle just inferior to foramen until needle touches maxilla.
- Inject 1-2cc anesthetic.
Intraoral Technique:
- Provide topical anesthetic to the mucosa superior to the maxillary canine.
- Dry the mucosa.
- Using your non-dominant hand, place your index finger on the infraorbital foramen and use your thumb to retract the lip.
- Insert your needle into the gingival reflection superior to the maxillary canine. Direct the needle superiorly until you reach the foramen (about halfway between the orbital rim and gingival reflection). Inject 3-5cc of anesthetic.
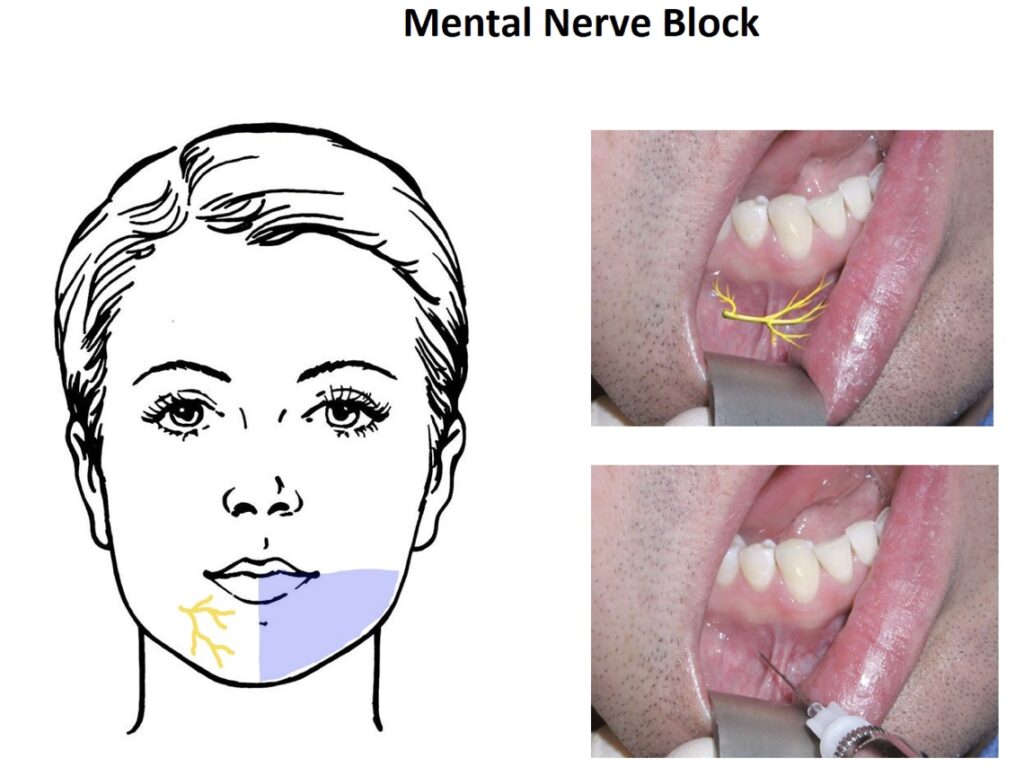
Mental Nerve Block
Anatomy:
- The mental nerve is a branch of the mandibular division of the trigeminal nerve.
- It exits the skull at the mental foramen. The mental foramen is vertically in line with the supraorbital foramen, infraorbital foramen, and pupil. It is horizontally in line with the middle of the body of the mandible.
- It provides sensation to the skin of the lower lip and chin.
Extraoral approach:
- Palpate the mental foramen using the above approach.
- Place a wheel superior to the foramen.
- Insert the needle through the wheel until it contacts the mandible.
- Inject 1-2cc of anesthetic.
Intraoral approach
- Provide topical anesthetic to the mucosa at the junction of the lower canine and first premolar (mouth can be open or closed).
- Dry the mucosa.
- Insert the needle inferiorly and posteriorly through the gingival mucosa.
- Advance ⅓ of the depth of the mandible body and make contact with the mandible.
- Inject 1-2 cc of anesthetic.
Occipital Nerves:
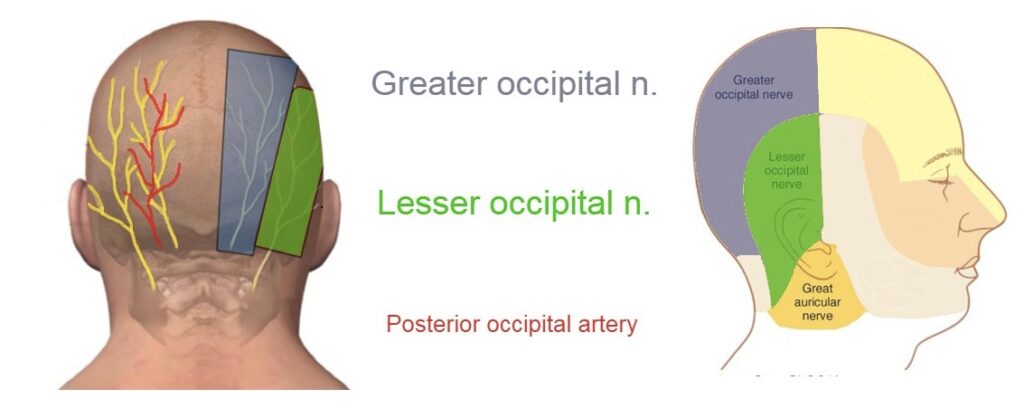
- Anatomy: The occipital nerves are a group of nerves that arise from C2-C3 and provide innervation to the posterior scalp and ear. They include the greater occipital nerve, the lesser occipital nerve, and the third occipital nerve.
- Indications: occipital neuralgia, cluster headache, occipital migraine
Greater occipital Nerve block:
Anatomy:
- The greater occipital nerve branches off C2 and provides sensory to the posterior neck up to the scalp vertex.
- The greater occipital nerve runs just medial to the posterior occipital artery.
Technique:
- Palpate the occipital protuberance and mastoid process. Draw an imaginary line between the two.
- The occipital artery can be palpable about ⅓ of the occipital protuberance.
- Inject a small amount of anesthetic to make a wheel over the occipital artery.
- Inject 1 ml of anesthetic 1-2mm to the left and right of the artery—aspirate before injection to avoid intravascular injection.
If the occipital artery cannot be palpated, divide the imaginary line between the mastoid process and external occipital protuberance into thirds. Infiltrate the middle third with 5-8cc of anesthetic (will also anesthetize the lesser occipital nerve)
Lesser occipital nerve block:
Anatomy:
- The lesser occipital nerve is a branch of the cervical plexus.
- It provides innervation to the skin between the skin and scalp, between the ear and the mastoid process.
- The lesser occipital nerve emerges from the middle third of the posterior border of the sternocleidomastoid muscle and travels superiorly towards the mastoid process.
Technique:
- Make a wheel just posterior to the mastoid process.
- Insert the needle through the wheel towards the posterior ear.
- Once the posterior ear is contacted, aspirate and inject anesthetic while pulling back towards the wheel to anesthetize the area between the mastoid process and the posterior ear.
Aurical Block:

Anatomy:
- The ear is innervated by two nerves.
- The auriculotemporal nerve innervates the anterior ear.
- The greater auricular nerve innervates the posterior ear.
Technique: This technique is a ring block and will anesthetize the entire ear.
-
- Insert the needle into the skin just inferior to the attachment of the ear lobe to the scalp.
- Advance the needle towards the tragus while aspirating. Inject 2-3cc of anesthetic while withdrawing.
- Redirect the needle posteriorly and superiorly aspirating while advancing. Inject 2-3 cc of anesthetic while withdrawing.
- Interior the needle into the skin just superior to where the ear’s helix attaches to the scalp.
- Advance the needle towards tragus aspirating while advancing. Inject 2-3cc of anesthetic while withdrawing.
- Redirect the needle posterior and inferiorly aspirating while advancing. Inject 2-3cc of anesthetic while withdrawing.
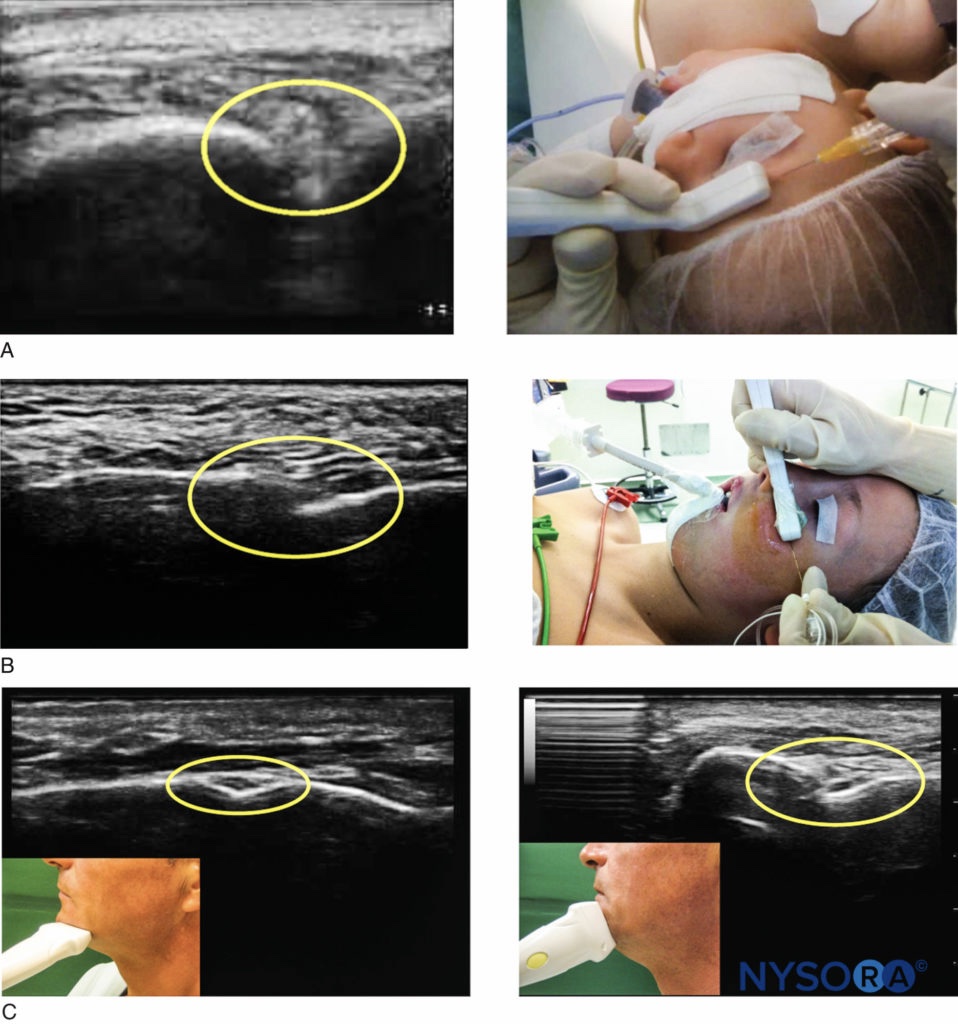
Ultrasound Guidance:
US guidance may lead to fewer complications (intravascular injection, vascular puncture, intraneural injection), higher success rate, shorter procedure time, and less total anesthetic used.5 Ultrasound guidance can be applied to all the techniques discussed above.
Technique:
- Identify the foramen using the landmark technique.
- Use a linear probe to confirm the location of the foramen.
- Use your non-dominant hand to hold the US probe and your dominant hand to insert the needle in the longitudinal axis and inject around the foramen (avoid injecting directly into the foramen, as increased pressure can result in nerve necrosis).
References:
- Tintinalies chapter 156.
- https://www.nuemblog.com/blog/occipital-nerve-block
- Chapter 156: Regional Nerve Blocks (Regional Anesthesia), Eric F. Reichman; Jehangir Meer
- Atlas of Pain Medicine Procedures. Sudhir Diwan, Peter S. Staats. Chapter 20: Periorbital Nerve Blocks (Supraorbital, Supratrochlear, and Infraorbital Nerves), Sanford Silverman. ©2021 McGraw Hill. All Rights Reserved
- Kasia Rubin, Denise Sullivan, Senthilkumar Sadhasivam. Are peripheral and neuraxial blocks with ultrasound guidance more effective and safe in children? Paediatr Anaesth. 2009 Feb;19(2):92-6.