Incidence: Spinal column injuries in blunt trauma varies from 2-6% (Kaji 2013)
C-Spine Injuries Table
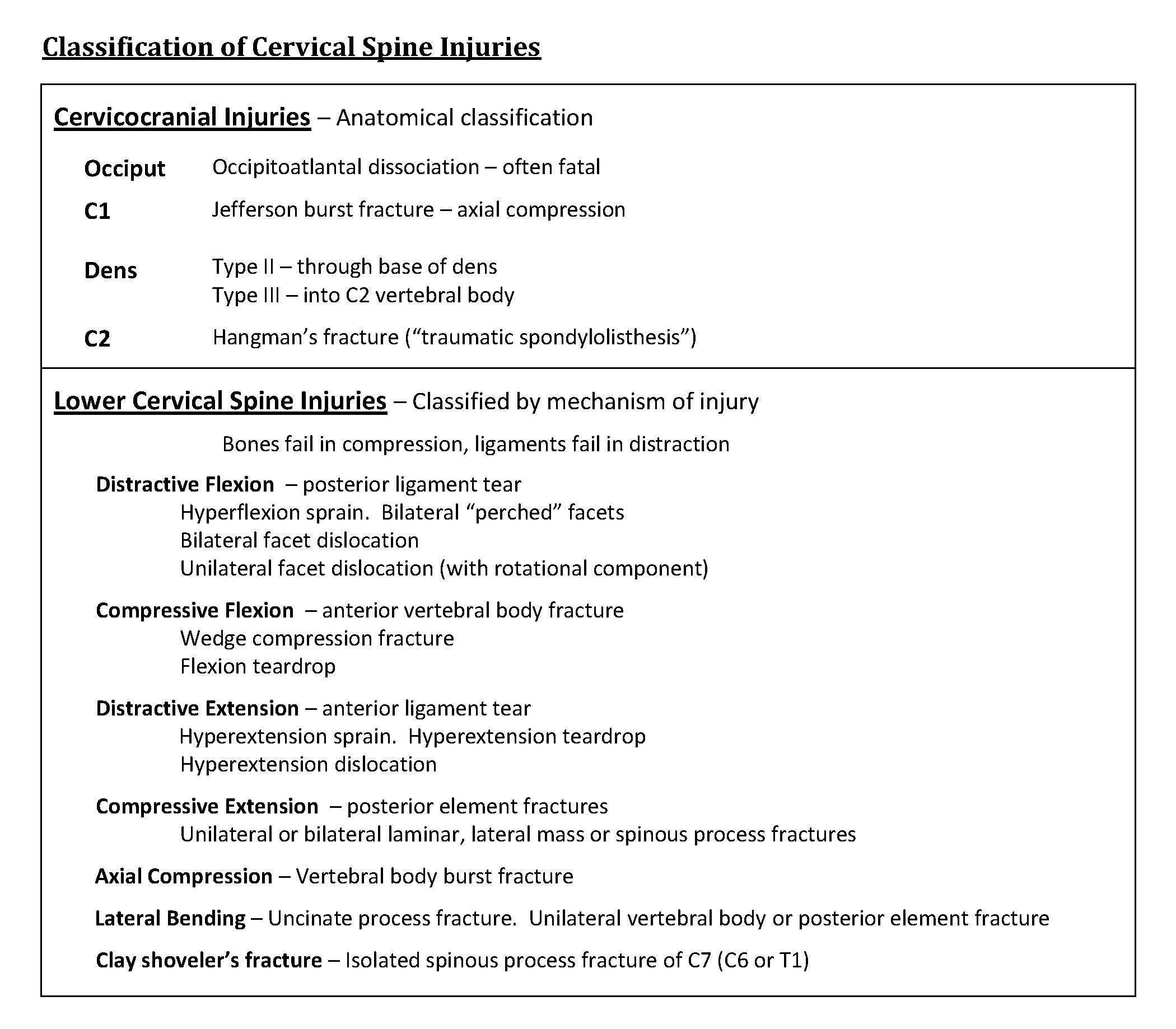
Classification: There are many different systems to organize cervical spine injuries. Furthermore, there exist a long listing of possible cervical spine injuries; this is not a complete listing. This post will only cover the most unstable and the most severe injuries.
Cervicocranial injuries (C1-C2) can be distinguished from lower cervical spine injuries (C3-C7). Cervicocranial injuries are classified by their anatomical location whereas lower cervical spine injuries are classified by their mechanism of injury (Schwartz 2008).
Jefferson burst fractures
- Definition: vertical force transmitted through the occipital condyles to C1 causes fractures in both the anterior and posterior arches with the lateral masses pushed laterally (bursts apart the ring of C1)
- Mechanism: axial compression
- Associated Neurologic Injury: Low incidence as fracture pieces tend to move away from the spinal cord; neurologic deficit can occur in the setting that a fractured piece compress part of the cord. Neurologic injury at this level is often fatal.
- Significant CT findings
- Sagittal: (figure1)If the transverse atlantal ligament is disrupted, there will be widening of the atlantodental interval (>3mm)
- Coronal: (figure 2) Lateral displacement of lateral masses
- Axial: (figure 3) Fractures in the anterior and posterior arches
Jefferson Burst Fracture CT Figures

Figure 1 (Sagittal): Transverse atlantal ligament is disrupted

Figure 2 (Coronal): Lateral displacement of lateral masses

Figure 3 (Axial): Fractures in the anterior and posterior arches
Dens fractures: Type II and Type III in Anderson-D’Alonzo classification
- Mechanism: multiple complex forces including hyperflexion, hyperextension, and rotational (Pope 2013)
- Associated Neurologic Injury: Variable depending on degree of displacement
- Type II dens fracture:
- Definition: Transverse fracture at the base of the dens
- Significant CT findings:
- Sagittal: (figure 4) fracture line through the dens
- Coronal: (figure 5) fracture not affecting body of C2
- Type III dens fracture
- Definition: Fracture through the dens extending to the body of C2
- Significant CT findings:
- Sagittal: (Figure 6) Fracture line through the body of C2
- Coronal: (Figure 7) Transverse fracture through C2 body
Hangman’s Fracture (Traumatic Spondylolisthesis of the axis)
- Definition: Fracture through the pars interarticularis of C2 with associated disruption of anterior longitudinal ligament, which can result in anterolisthesis of the vertebral body. (figure 8)
 Mechanism: hyperextension and compression—this is often recreated by motor vehicle collisions in which the patient’s chest hit the steering wheel and head launches forward and is stopped by the windshield. In judicial hanging, the mechanism is hyperextention with distraction and is fatal.
Mechanism: hyperextension and compression—this is often recreated by motor vehicle collisions in which the patient’s chest hit the steering wheel and head launches forward and is stopped by the windshield. In judicial hanging, the mechanism is hyperextention with distraction and is fatal.- Associated Neurologic Injury: Due to the increased width of the spinal canal at the cervicocranium, neurologic injury is uncommon depending on the degree of displacement of the vertebral body (Schwartz 2008). Complete spinal cord syndrome can result in severe anterolisthesis of the vertebral body, which is often fatal at this level.
- Significant CT findings:
- Sagittal: (figure 9) Fracture through the pars interarticularis of C2
- Coronal: (figure 10) Fracture through the pars interarticularis of C2 (Schwartz 2008).
- Axial: (figure 11) Fracture through the pars interarticularis of C2
C2 Fracture Figures

Figure 4 (Sagittal): Fracture line through the dens

Figure 5 (Coronal): Fracture not affecting body of C2

Figure 6 (Sagittal): Fracture line through the body of C2

Figure 7 (Coronal): Transverse fracture through C2 body

Figure 8: Fracture through Pars interarticularis of C2 with associated disruption of anterior longitudinal ligament

Figure 9 (Sagittal): Fracture through the pars interarticularis of C2

Figure 10 (Coronal): Fracture through the pars interarticularis of C2

Figure 10 (Axial): Fracture through the pars interarticularis of C2
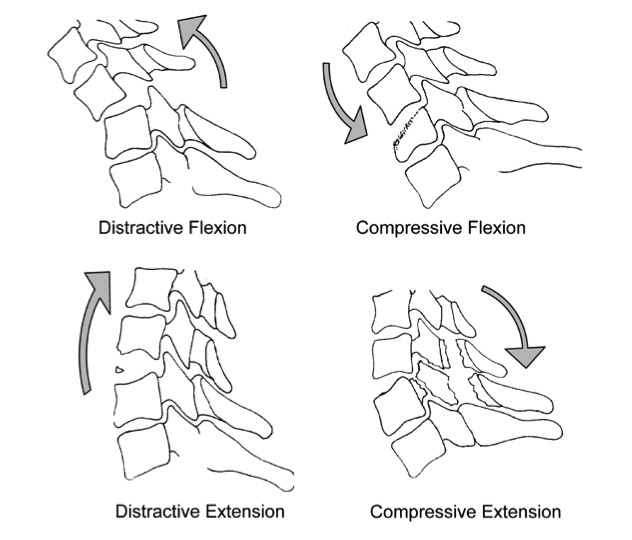 Lower Cervical Spine – Categorized by major mechanisms: distractive flexion, compression flexion, distractive extension and compressive extension
Lower Cervical Spine – Categorized by major mechanisms: distractive flexion, compression flexion, distractive extension and compressive extension
Flexion Teardrop Fracture
- Definition: Fragmentation of the vertebral body and disruption of all ligamentous structures as well as intervertebral disks as a result of 2 vertebral bodies compressing together
- Mechanism: Compressive-flexion, often presents as diving into shallow pool
- Associated Neurologic Injury: anterior cord syndrome (quadriplegia with loss of pain, touch and temperature sensation, but intact proprioception)
- Significant CT findings: (Pope 2013)
- Sagittal: (Figure 12) Retrolisthesis of the superior vertebral body fragment into the spinal canal and the anterior inferior vertebral body fragment represents the “teardrop” in its namesake
- Axial: (Figure 13) Comminuted fracture of the vertebral body with increased width of the facet joints
Bilateral Interfacetal Dislocation
- Definition: Generally a purely ligamentous injury with disruption of all ligamentous structures (3 columns) causing displacement of the articular pillars anteriorly and superiorly atop the superior articular facet of the inferior vertebrae (Pope 2013).
- Mechanism: distractive flexion
- Associated Neurologic Injury: complete cord syndrome if anteriolisthesis of the vertebral body is substantial (>50% of vertebral body diameter)
- Significant CT findings:
- Sagittal:
- Mid-sagittal: (figure 14) anterolisthesis of the vertebral body usually more than half of the vertebral body diameter
- Parasagittal: (figure 15) anterior and superior displacement of the articular facets
- Axial: (figure 16) Reverse hamburger sign. The “buns” of the hamburgers appear to be inversed (Pope 2013).
- Sagittal:
 Hyperextension Dislocation: also called hyperextension sprain
Hyperextension Dislocation: also called hyperextension sprain
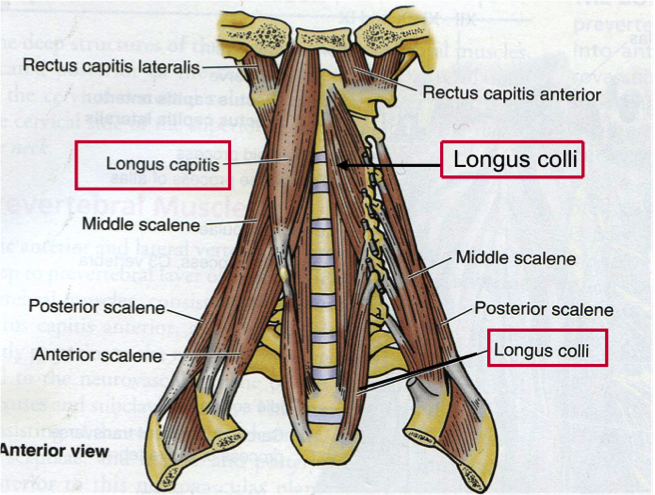
- Definition: Disruption of all ligamentous structures in addition to injury of the longus colli and longus capitis muscles pushing the vertebrae posteriorly compressing the spinal cord against the ligamentum flavum (Pope 2013).
- Mechanism: Distractive-extension. Usually cause by force applied to face causing hyperextension of neck such as slipping and hitting chin on sink while falling down (Pope 2013).
- Associated Neurologic Injury: Central cord syndrome (loss of motor and sensation in upper extremities and urinary retention)
- Significant CT findings:
- Sagittal: (figure 17) Retrolisthesis of the vertebral body may not be present. Anterior disk space widening is key. Also commonly found is diffuse prevertebral soft tissue swelling.
Bilateral pedicolaminar fractures
- Definition: Fracture through bilateral pedicles and lamina causing the lateral masses to become floating islands. Very uncommon injury
- Mechanism: Compressive extension
- Significant CT findings:
- Axial: (Figure 18 and figure 19) Look for fractures of both the pedicle and lamina. The lateral masses may be crushed with fracture fragments protruding into the vertebral canal.
Lower Cervical Spine Injuries Figures

Figure 12 (Sagittal): Retrolisthesis of the superior vertebral body fragment into the spinal canal and the anterior inferior vertebral body

Figure 13 (Axial): Comminuted fracture of the vertebral body

Figure 14 (Mid-Sagittal): Anterolisthesis of the vertebral body

Figure 15 (Parasagittal): Anterior and superior displacement of the articular facets

Figure 16 (Axial): Reverse hamburger sign

Figure 17 (Sagittal): Retrolisthesis of the vertebral body may not be present. Anterior disk space widening is key

Figure 18 (Axial)

Galli RL, Spaite DW, Simon RR: Emergency Orthopedics: The Spine. McGraw-Hill, 1989.
Kaji A, Hockberger RS, Spinal column injuries in adults: definitions, mechanisms and radiographs. In: UpToDate, Moreira ME (ed), UpToDate, Waltham, MA. (Accessed on 12/23/15)
Pope TL Jr, Harris JH. Chapter 5. Cervical Spine Injuries. In: Pope TL. eds. Harris & Harris’ The Radiology of Emergency Medicine. Philadelphia, PA: Lippincott Williams & Wilkins.
Schwartz DT. Section 5. Cervical Spine. In: Schwartz DT: Emergency Radiology: Case Studies. New York, NY: McGraw-Hill, 2008. http://accessemergencymedicine.mhmedical.com/ (via NYU Health Sciences Library)
