Definition: Interruption of the normal conduction system leading to aberrant conduction and an abnormal QRS morphology
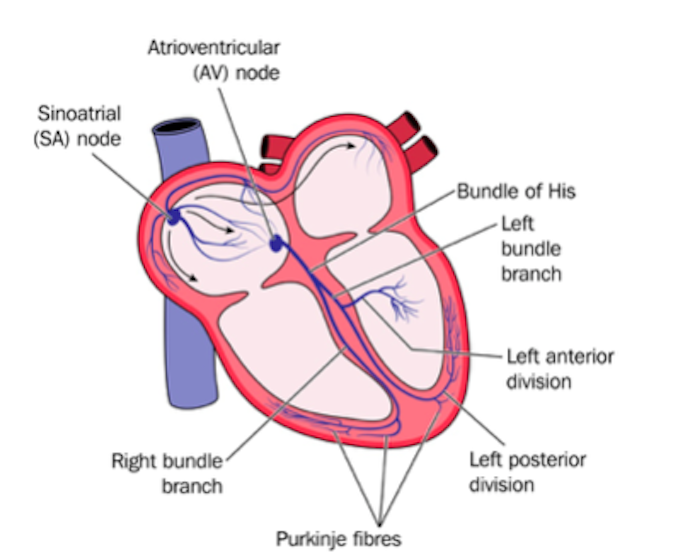
Anatomy: At the AV node, conduction splits into the right and left bundle branches. The left bundle branch is composed of anterior and posterior branches.
Right Bundle Branch Block (RBBB)
Physiology
- Normally, the right bundle depolarizes the right ventricle (RV)
- In a RBBB, the right bundle does not activate. The right ventricle is instead depolarized by spread of impulse from the left bundle, through the left ventricle (LV) and then to the RV
- This pattern of electrical spread creates an aberrant QRS morphology
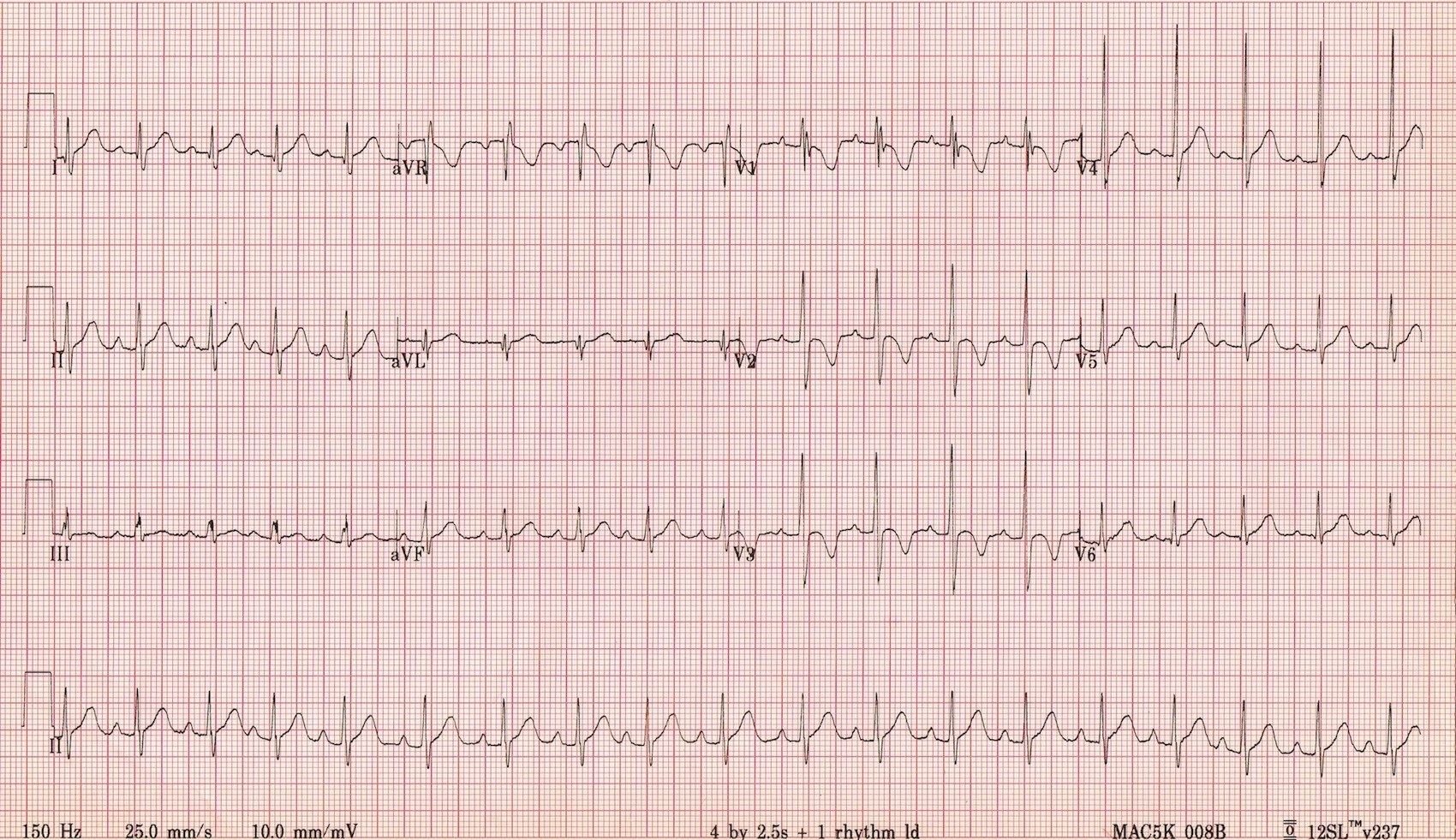
RBBB Criteria
- Rhythm is supraventricular in origin
- QRS duration > 110 msec (some criteria state > 120 msec)
- Terminal R wave in lead V1 giving an RSR’ morphology (i.e. “Rabbit Ears”)
- Wide terminal S wave in leads I, aVL, V5 and V6
RBBB (LITFL)
Note: A incomplete RBBB, defined as a RBBB morphology with a QRS < 100 msec, can be pathologic (i.e. in right heart strain) or a normal variant (seen in up to 10% of the general population)
Incomplete RBBB (LITFL)
Left Bundle Branch Block (LBBB)
Physiology
- The left bundle is composed of two fascicles (the left anterior and the left posterior fascicle)
- Normally, the left bundle depolarizes the left ventricle
- In a LBBB, the left bundle does not activate. The left ventricle is, instead, depolarized by spread of impulse from the right bundle through the RV and then to the LV.
- This pattern of electrical spread creates an aberrant QRS morphology
- The left bundle has two fascicles (anterior and posterior) and either (or both) can have a conduction abnormality
LBBB Criteria
- Rhythm is supraventricular in origin
- QRS duration > 120 msec
- QS or rS morphology in lead V1 + V2
- Broad, dominant monomorphic R wave in lead I, aVL, V5 and V6
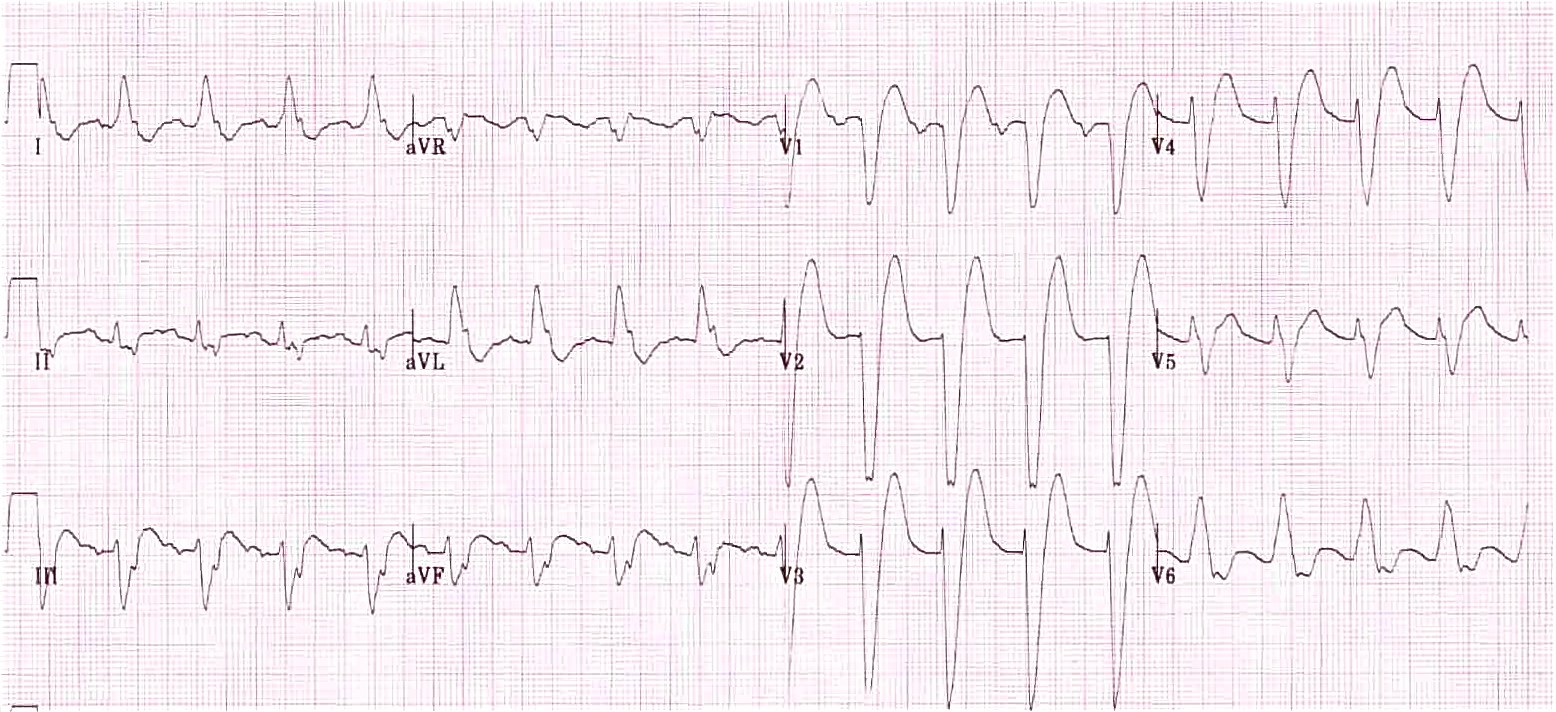
LBBB (LITFL)
Fascicular Blocks
Left Anterior Fascicular Block (LAFB aka left anterior hemi-block)
- Blocking the left anterior fascicle results in LV depolarization via the left posterior fascicle which inserts into the infero-septal wall of the LV
- Produces small R waves in II, III, aVF
- Produces tall R waves in left-sided leads and deep S waves in the inferior leads
- LAFB EKG Criteria
- Left axis deviation (QRS up in I, down in II + aVF)
- Slight prolongation of the QRS complex (but < 120 msec)
- Small q waves and large R waves (qR complexes) in leads I and aVL
- Small r waves and large S waves (rS complexes) in leads II, III + aVF
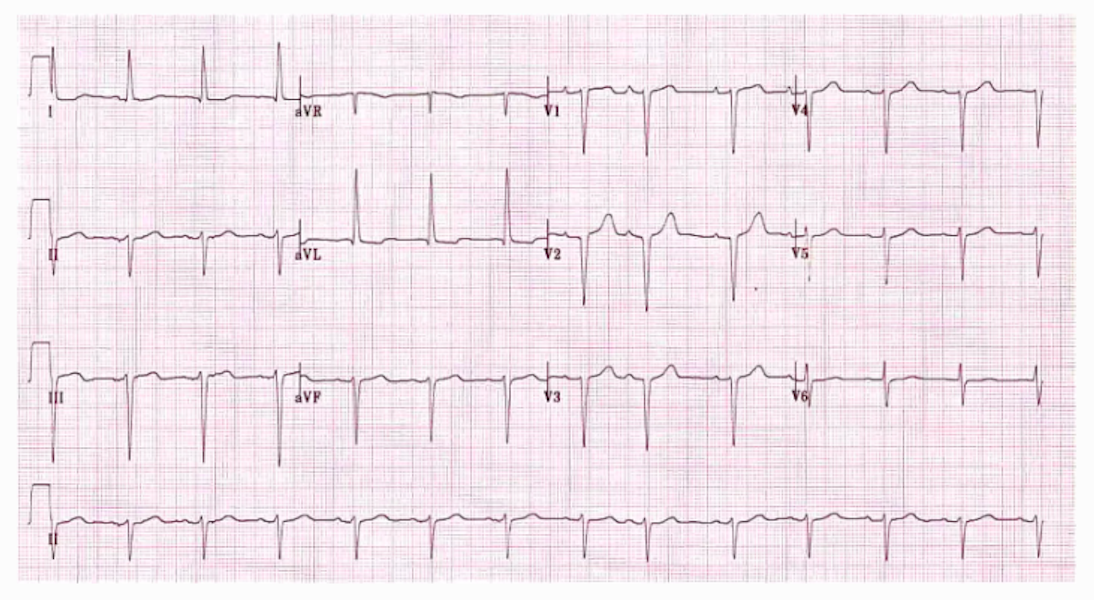
LAFB (LITFL)
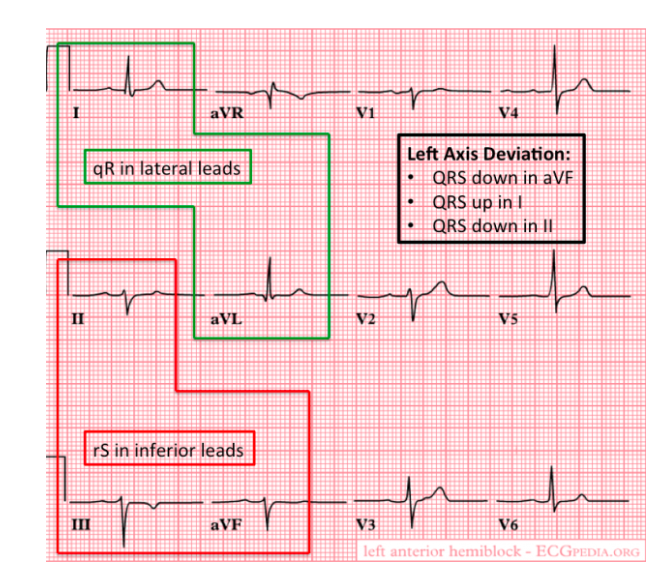
LAFB Annotated (REBEL EM)
Left Posterior Fascicular Block (LPFB aka left posterior hemi-block)
- Blocking the left posterior fascicle results in LV depolarization via the left anterior fascicle which inserts into the upper, lateral wall of the LV
- LPFB is much less common than LAFB and the LAFB typically occurs with a RBBB (bifascicular block)
- LPFB EKG Criteria
- Right axis deviation (RAD) (QRS up in III + aVF, down in I)
- Slight prolongation of the QRS complex (but < 120 msec)
- qR complexes in leads II, III + aVF
- rS complexes in leads I + aVL
- No evidence of RV hypertrophy
- No evidence of other cause of right axis deviation
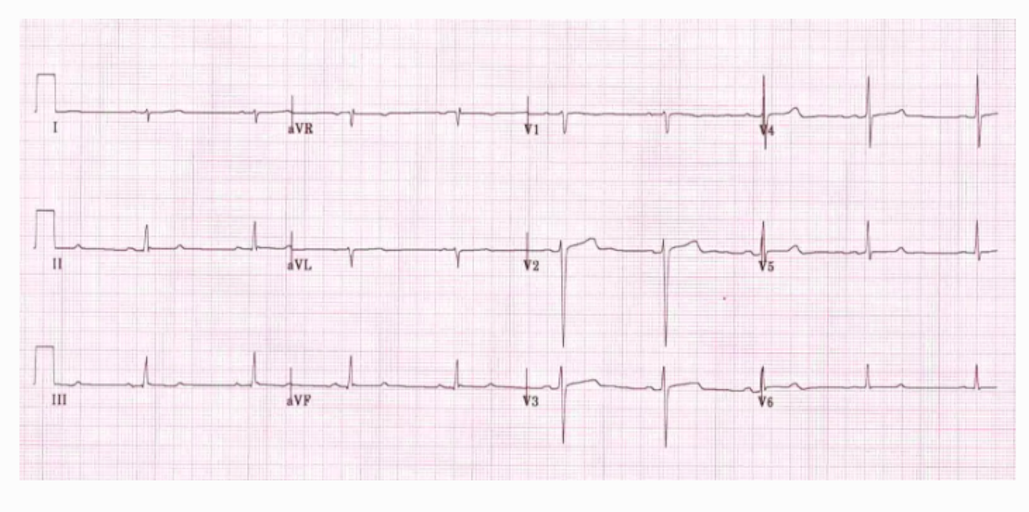
LPFB (LITFL)
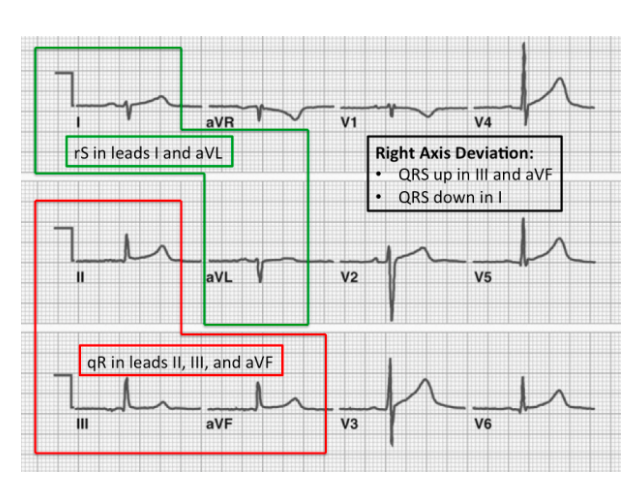
LPFB Annotated (REBEL EM)
- Causes of RAD
- LPFB
- Old lateral myocardial infarction
- Acute pulmonary hypertension (e.g. pulmonary embolism)
- Chronic pulmonary hypertension
- Sodium channel blocking drugs
- Hyperkalemia
- Right ventricular hypertrophy
- Misplaced leads
|
Axis Deviation |
II, III + aVF |
I + aVL |
|
|
LAFB |
Left Axis Deviation |
rS Complexes |
qR Compexes |
|
LPFB |
Right Axis Deviation |
qR Complexes |
rS Complexes |
Read More
REBEL EM: Bundle Branch Blocks: 101
LITFL: Left Anterior Fascicular Block
LITFL: Left Posterior Fascicular Block
LITFL: Right Axis Deviation

Thank you for sharing this information! Very clear and informative for a spouse, seeking to understand her husband’s LBBB.