Definition
- Rupture of the biceps tendon, most frequently at the proximal end of the long head of the bicep
- Rupture of the triceps tendon, most frequently at the insertion of the medial or lateral head to the olecranon
 Anatomy
Anatomy
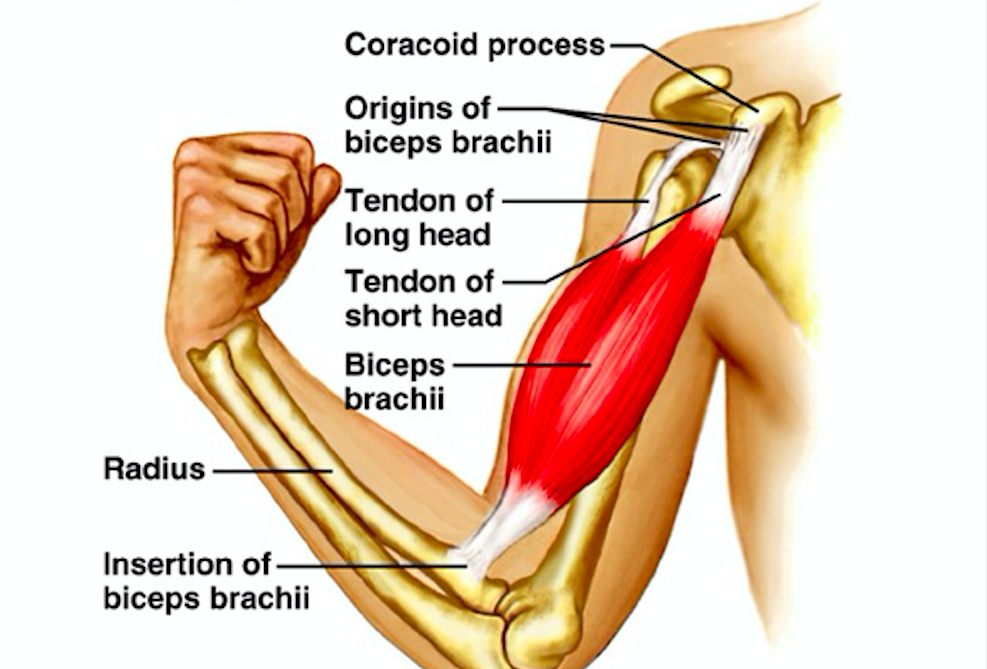
- Biceps Tendon
- The biceps muscle is divided into two tendons proximally:
- The short head of the bicep inserts at the coracoid process. It is rarely a source of pain and helps with arm flexion.
- The long head of the bicep runs over the top of the humerus and inserts at the glenoid. It is primarily responsible for arm abduction and is a common source of anterior shoulder pain.
- The distal tendon inserts at the radial tuberosity
Triceps Tendon Anatomy (www.musculoskeletalkey.com)
- The biceps muscle is divided into two tendons proximally:
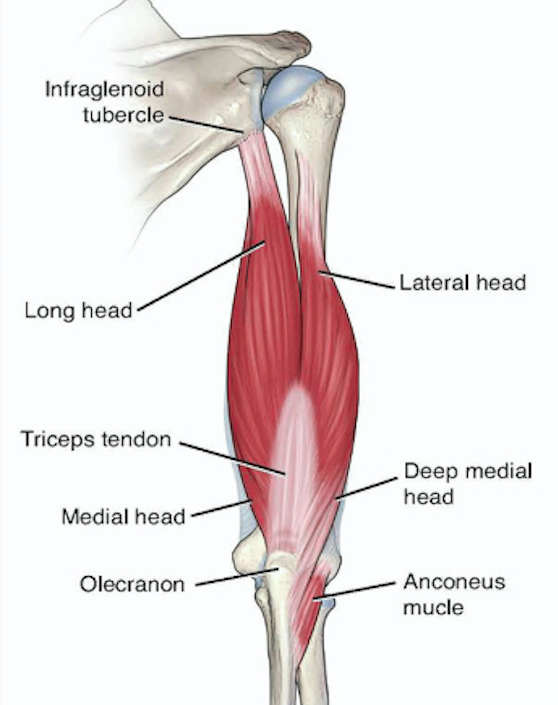
- Triceps Tendon
- The triceps muscle has three heads:
- The long head arises from the infraglenoid tubercle, with the tendon attaching to the glenoid cavity.
- The lateral head attaches to the upper margin of the radial grove of the humerus.
- The medial head originates below the lateral margin of the radial groove and inserts at the posterior surface of the humerus
- Distally, the triceps tendon inserts at the olecranon process
- The triceps muscle has three heads:
Epidemiology
- Biceps Tendon Rupture
- Location (Clayton 2008)
- Proximal end of the long head of the bicep at the glenoid – 96%
- Distal along the radial tuberosity – 3%
- Short head of the bicep – 1%
- Usually seen in older patients – median age 46
- Risk factors include recurrent tendinitis, a history of a rotator cuff injury, a contralateral biceps tendon rupture, age, poor conditioning and rheumatoid arthritis (Harwood 2005)
- Location (Clayton 2008)
- Triceps Tendon Rupture
- The least common of all tendon injuries. Accounts for less than 1% of all tendon ruptures within the upper extremity
- Most commonly occurs at the insertion of the medial or lateral head to the olecranon (Khiami 2012)
- Typically occurs in males, with ages 30-50 being the most common
- Risk factors include anabolic steroid use, local steroid injections for bursitis, oral steroid use, renal disease, diabetes and familial tendinopathy (Dunn 2017)

Popeye Deformity – Proximal Biceps Rupture (NPR.org)
Presentation
- Biceps Tendon Rupture
- Mechanism
- Fall on an outstretched hand or after lifting something heavy
- Can occur after routine athletic activities (i.e. throwing a football, taking a slap shot while playing hockey)
- Patients may complain of anterior shoulder pain and/or pain radiating down the region of the biceps
- Patients will often hear an audible pop or snap
- Physical Exam
- Tenderness with palpation over the biceps groove

Reverse Popeye Deformity – Distal Biceps Tendon Rupture (orthobullets.com)
(worse with internal rotation of arm)
- Difficulty supinating arm, may or may not have difficulty flexing arm
- “Popeye” muscle deformity
- Rupture of the proximal tendon of the biceps results in the muscle collecting distally.
- Reverse Popeye deformity (seen in distal tears)
- Tenderness with palpation over the biceps groove
- Mechanism
- Triceps Tendon Rupture
- Mechanism
- Typically occurs from forced bending of the elbow during a pushing activity
- Unlike biceps tendon ruptures, triceps tendon ruptures are almost always traumatic, as they require a large amount of force
- May occur after weightlifting or playing a contact sport such as football
- Patients often hear a pop with sudden acute pain along the course of the rupture

Olecranon Defect – Triceps Tendon Rupture (www.drdavidgeier.com)
- Patients will have difficulty extending their elbow
- Physical Exam
- There will typically be a noticeable defect just above the olecranon
- Modified Thompson’s Test
- Elbow is flexed to 90 degrees and arm is abducted
- Examiner squeezes triceps muscle below and observes for elbow extension
- If none is present, a complete tear is likely
- Easy to misdiagnose complete tear as swollen elbow can limit patient’s ability to extend
- There will typically be a noticeable defect just above the olecranon
- Mechanism
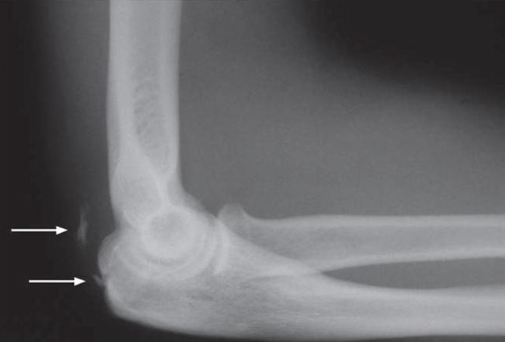
“Flake” Sign (www.orthobullets.com)
Imaging
- Obtain AP and lateral X-rays of the elbow with suspected triceps tendon ruptures, as they are typically associated with avulsion injuries
- “Flake sign”:
- Lateral radiographs of the elbow showing an avulsion fracture where the triceps insert at the olecranon
- “Flake sign”:
- MRI is the gold standard to determine severity and location of the tear for both biceps and triceps tendon ruptures but can be deferred to outpatient follow up
ED Management
- Provide analgesia
- Close follow up with orthopedics (within 1 week)
- Cases of isolated biceps or triceps tendon ruptures can be discharged from the ED with supportive care measures (rest, ice, analgesia, sling). In a community hospital without an in-house orthopedic surgeon, these patients do not warrant an emergent ortho consult in the ED
- A triceps tendon rupture with an associated avulsion injury warrants either ED ortho consult or very close (24-48 hours) follow up, as these patients require surgical repair within 2 weeks of injury
Prognosis (Leslie 2002)
- Biceps Tendon Rupture
- The main indication for operative repair is restoration of supination strength. However, patients may also elect to have operative treatment for cosmetic reasons.
- If supination strength and/or cosmetics are not important to the patient, non-operative treatment can be considered.
- Flexion and supination strength generally return to near baseline levels. Patients can expect to return to normal functioning between 4-9 months after surgery.
- The most common complication is a neuropraxia of the lateral antebrachial cutaneous nerve.
- Triceps Tendon Rupture
- Complete tears are debilitating and should be repaired surgically.
- Partial tears >50% with significant weakness should also be repaired surgically.
- Partial tears in which patients retain their ability to extend their elbow against gravity can be treated non-operatively with physical therapy and NSAIDs.
- Patients can expect to regain almost full range of motion of the elbow, with possible loss of a few degrees of elbow extension.
- Patients can expect to return to full activities 12 weeks after surgery.
- Complications include elbow stiffness and ulnar nerve injury, the latter of which is very rare.
- Generally, patients treated nonoperatively for biceps and triceps tendon ruptures have weaker supination/flexion and elbow extension, respectively, compared to patients treated surgically.
Take Home Points
- Biceps tendon rupture can be a result of trauma or overuse, but can also present after relatively routine activities. Triceps tendon ruptures are almost always traumatic and typically require a large amount of force
- Patients typically hear a popping sound and will present with difficulty supinating and/or flexing their arm (biceps) or extending their elbow (triceps)
- For suspected triceps tendon rupture, elbow X-rays should be obtained to evaluate for an avulsion injury. However, non-emergent MRI is the gold standard for both bicep and triceps tendon ruptures
- Patients can be discharged from the ED but warrant close follow-up with an orthopedic surgeon
Read More
OrthoInfo: Biceps Tendon Tear at the Shoulder
Orthobullets: Biceps Tendonitis
Orthobullets: Distal Biceps Avulsion
Orthobullets: Triceps Rupture
References
Clayton RA, Court-Brown CM. The epidemiology of musculoskeletal tendinous and ligamentous injuries. Injury. 2008. 39(12): 1338. PMID: 19036362
Dunn JC et al. Triceps Tendon Ruptures: A systematic Review. Hand. 2017; 12(5): 431-438. PMID: 28832209
Harwood MI, Smith CT. Superior labrum, anterior-posterior lesions and biceps injuries: diagnostic and treatment considerations. Prim Care. 2005; 31(4): 831. PMID: 15544823
Kelly MP et al. Distal Biceps Tendon Ruptures: An Epidemiological Analysis Using a Large Population Database. Am J Sports Med. 2015; 43(8): 2012-7. PMID: 26063401
Khiami F et al. Distal partial ruptures of triceps brachii tendon in an athlete. Orthopaedics & Traumatology: Surgery & Research. 2012; 98(2): 242-246. PMID: 22381568
Leslie BM, Ranger H. (2002) Biceps Tendon and Triceps Tendon Ruptures. In: Baker C.L., Plancher K.D. (eds) Operative Treatment of Elbow Injuries. Springer, New York, NY.