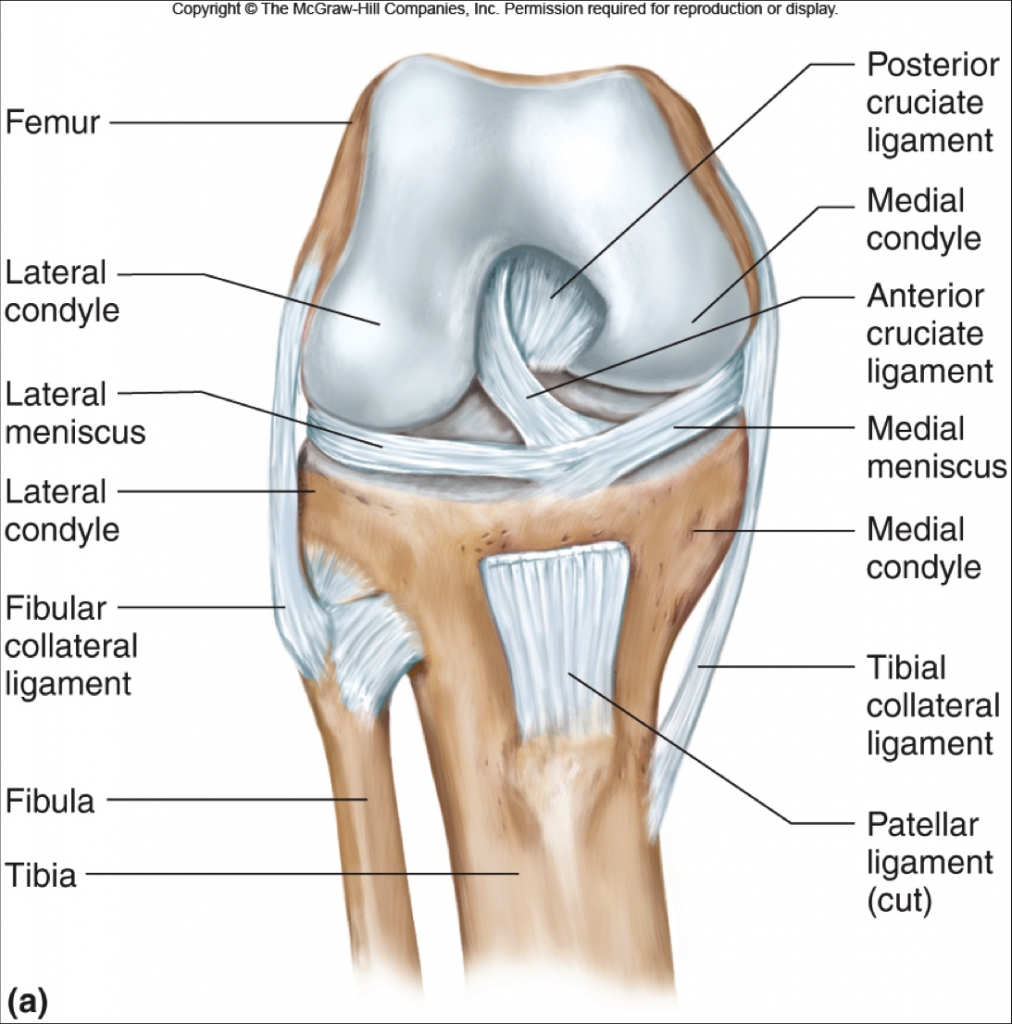
Knee Ligament Anatomy (thesistut.com)
Definition: Sprain or tear of the anterior cruciate ligament (ACL).
Mechanism of Injury (Boden 2000)
- High energy (Motor Vehicle Accident and Contact sports)
- Direct blow to the knee causing hyperextension or valgus deformity
- Can also be seen in sports, as in football with a tackle into the leg with the foot planted
- Direct blow in MVA, often missed in primary evaluation in multi-trauma cases
- Low energy (non-contact sports injuries)
- Sudden deceleration or direction change in a running or jumping athlete
- Sudden rotation or valgus stress to the knee, with minimal flexion and internal rotation.
Epidemiology (Miyasaka 1991, Agel 2016)
- Most commonly injured knee ligament, 100,000-200,000 ruptures per year
- Annual incidence of 1 in 3500
- Most commonly from non-contact athletic injuries
- Largest number in the US are from football, although those are more often contact injuries
- More common in women by percentage although not overall number
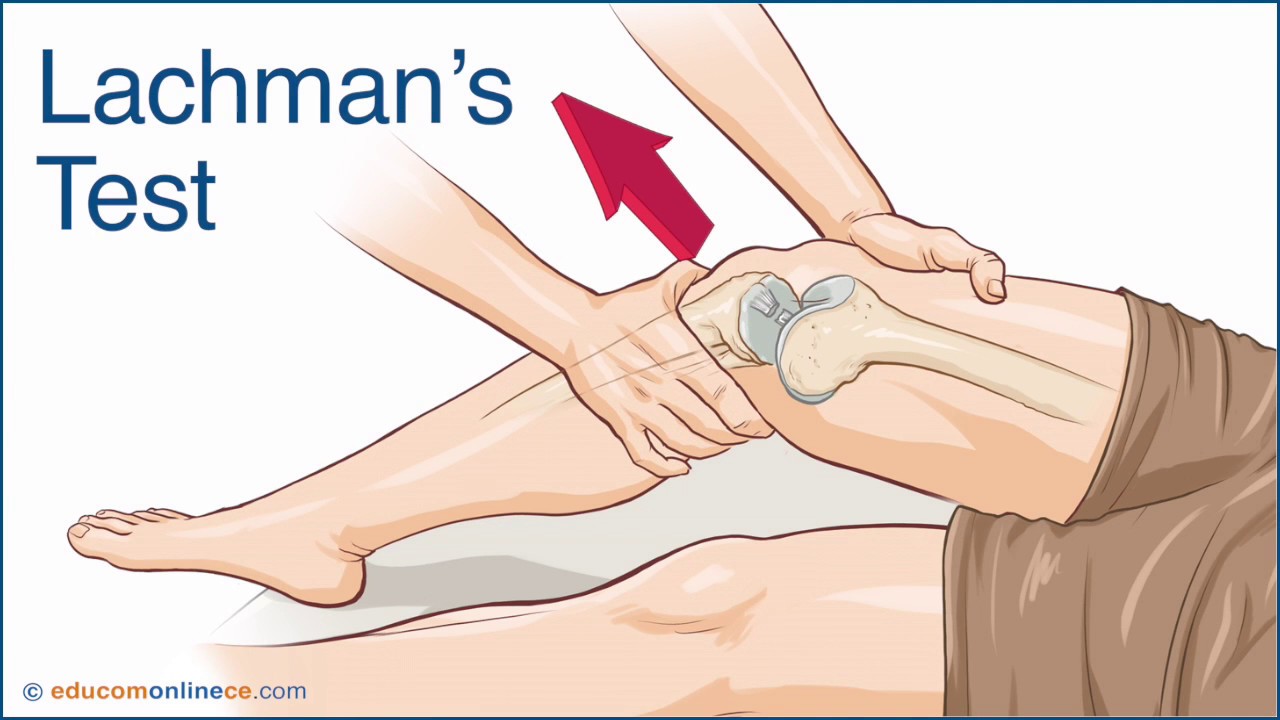
Lachman’s Test
Presentation
- History
- Usually report a “popping” sensation at the time of injury (Boden 2000)
- Acute swelling
- Knee instability, especially with squatting, pivoting, lateral movement (OrthoInfo 2017)
- Physical Examination
- Always compare to the unaffected knee for comparison. (OrthoInfo 2017)
- Often exam is best immediately after the injury, as swelling and pain may increase after the injury
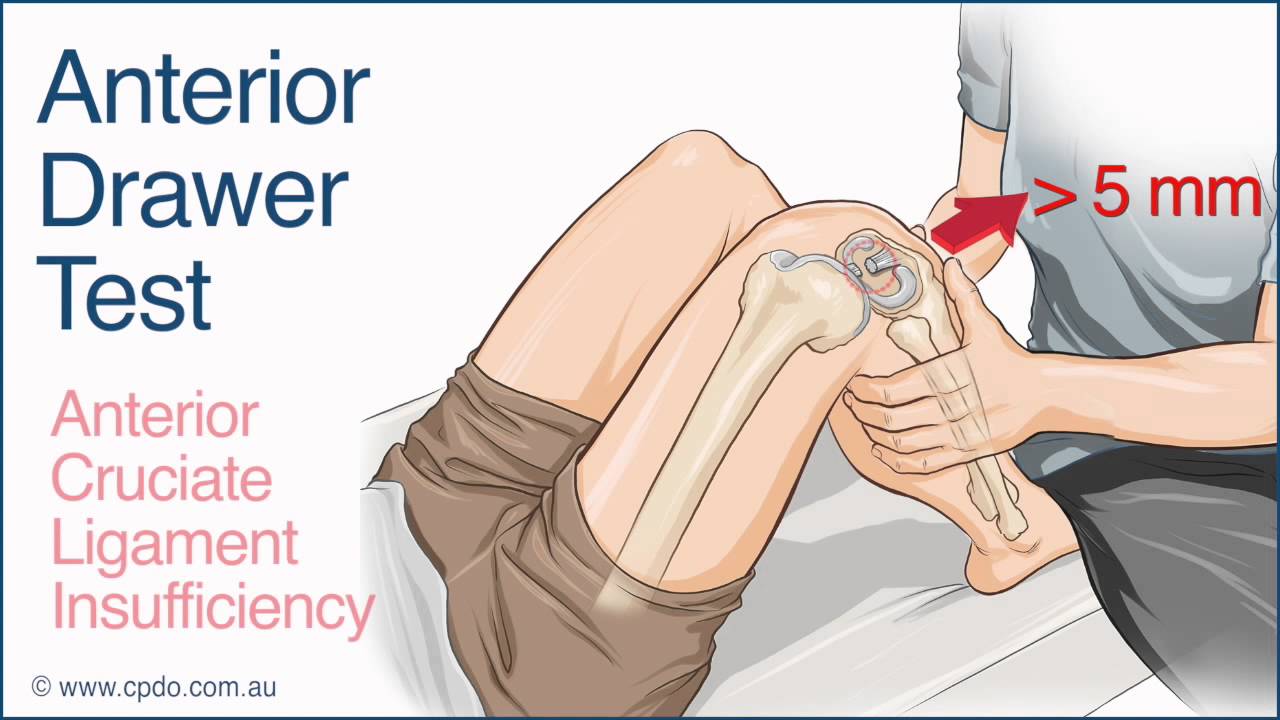
Anterior Drawer Test
- Lachman test
- Place knee in 30 degrees flexion, stabilize distal femur and pull proximal tibia anteriorly
- Positive with anterior translation of tibia
- Anterior drawer test
- Patient lies supine with knee flexed at 90 degrees, tibia pulled anteriorly
- Positive with anterior translation of the tibia
- Always compare to the contralateral side as many people have physiologic laxity
- Great test in chronic injuries, but performs worse in acute injuries
- Pivot Shift Test (Video Link)
- Difficult to perform if patient is guarding. Requires full cooperation and relaxation
- Start with knee in extension, internally rotate the tibia while placing valgus stress on the knee causing the joint to sublux, then flex the knee, causing a reduction
- Positive test with a “clunk” of the tibia as it reduces with flexion
- Lever Test (Video Link)
- Newly established test (Lelli 2016)
- The original study found it to be 100% sensitive and specific in partial and complete tears
- Subsequent studies showed 98% sensitive under anesthesia, 96% without
- This would make it more sensitive and specific than Lachman, especially for partial tears
- Further study is needed, but this is a very promising diagnostic test
Likelihood Ratio Comparisons for ACL Physical Exam Maneuvers (Benjaminse 2006, Lelli 2016)
| Lachman | Anterior Drawer* | Pivot Shift | Lever | |
| Sensitivity | 85 | 92 | 24 | 98 |
| Specificity | 94 | 91 | 98 | 100¢ |
| +LR | 14.16 | 10.2 | 12 | ∞ |
| -LR | 0.16 | 0.09 | 0.78 | 0 |
*Anterior Drawer values for chronic tear only, does not do as well for acute tear ¢Lever Test values based on 2 studies only, limited data
-
- Posterior Collateral, Medial Collateral and Lateral Collateral Ligaments
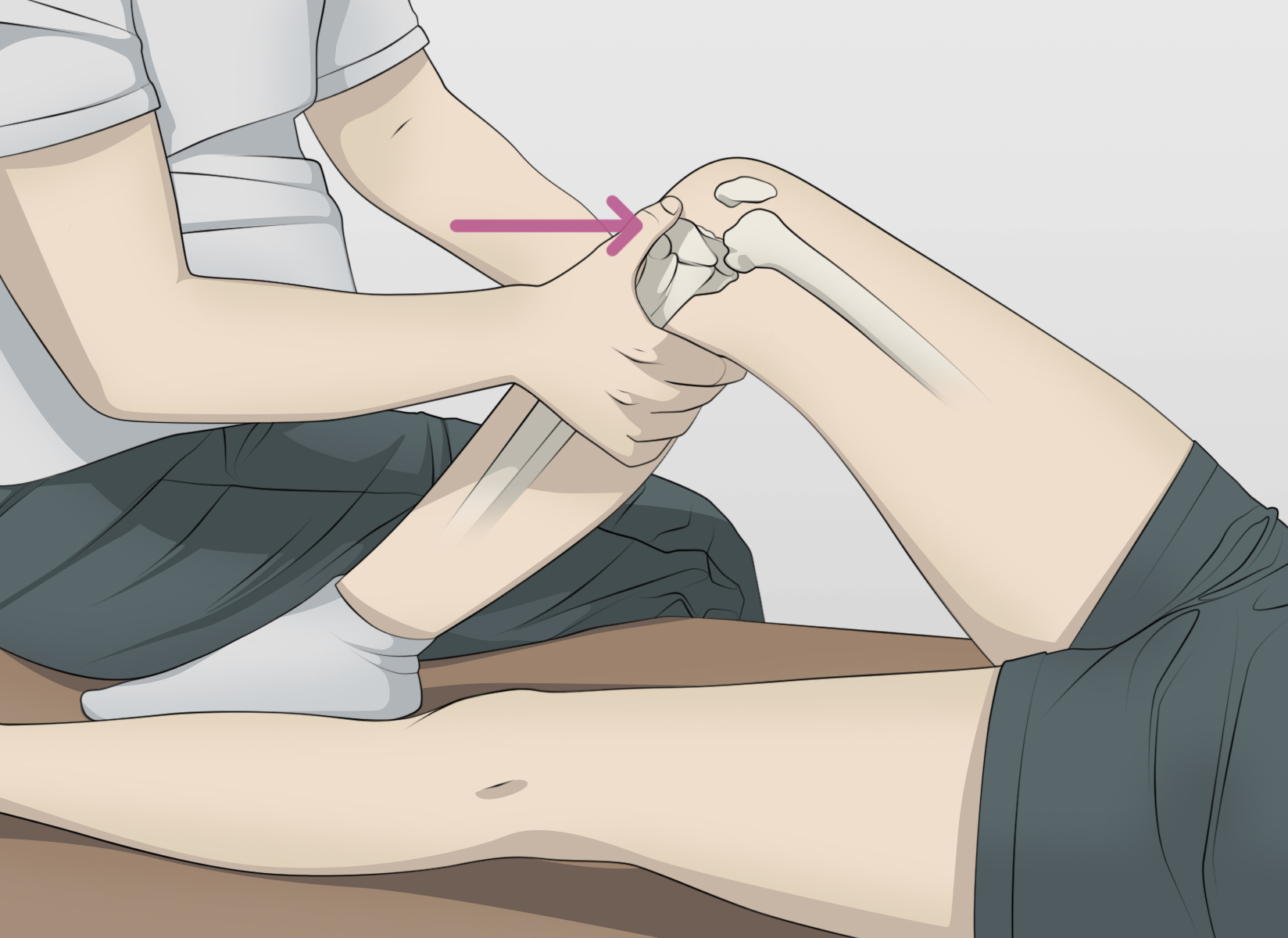
Posterior Drawer Test (medisavvy.com)
- Concomitant PCL/MCL/LCL injuries are common
- PCL Injuries
- ACL exams can be falsely positive with PCL injury, as the knee may have a posterior lag, and the return to neutral can be confused for an anterior translation
- Posterior drawer test is similar to anterior drawer but with posterior translation of the tibia
- MCL/LCL injuries
-
- Assessed with gradual varus/valgus stress to the knee
- Always compare to the contralateral knee as many patients, particularly children, may have some baseline laxity
- Valgus Stress Video
- Varus Stress Video
-
- Posterior Collateral, Medial Collateral and Lateral Collateral Ligaments
Classification
- Always important to note if the injury is isolated or associated with damage to another structure, such as the cartilage, meniscus, or other ligaments (common in 50% of ACL injuries)
- Grade 1 sprain: mild damage to the ligament, slightly stretched but able to keep knee joint stable
- Grade 2 sprain: the ligament is stretched enough to be loose, otherwise known as a partial tear.
- Grade 3 sprain: complete tear of the ligament, into two pieces, with knee joint instability.
Imaging
- Plain Radiographs
- Cannot evaluate ligamentous injuries
- Often performed after acute knee trauma to rule out bony injury but usually, unnecessary
- MRI
- Most commonly used in the US
- Performance characteristics (Crawford 2007)
- Sensitivity 86.5%
- Specificity 95.2%
- (+) Likelihood ratio: 18.02
- (-) Likelihood ratio: 0.14
- Typically performed on outpatient basis
- Ultrasound
- More common in Europe
- Performance Characteristics (Skovgaard 2000)
- Sensitivity 88%
- Specificity 98%
- (+) Likelihood ratio: 44.0
- (-) Likelihood ratio: 0.12
ED Management
- There is no need for emergency intervention in an isolated ACL injury
- Supportive Care
- Rest, Ice, Compression, and Elevation
- Analgesia
- Crutches for comfort if needed
- Knee immobilizer brace if unstable for comfort in the acute phase
- Long term use of knee immobilizer associated with muscle atrophy and stiffening of joint leading to prolonged recovery
- Patients will likely be switched to hinged brace by orthopedics on follow up
- Referral to orthopedic surgery
- May obtain delayed MRI
- no indication for urgent MRI
- Image quality may improve as swelling decreases
- Surgical options: Patellar tendon graft, hamstring tendon graft, and allograft
- May obtain delayed MRI
Prognosis (Ardern 2014)
- Prognosis depends on surgical management.
- Young, active patients typically get surgical repair
- 81% of reconstructed patients returned to some athletic activity
- 65% regain preinjury levels of competition
- 55% high level athletes return to competition
- Increased risk for osteoarthritis (although how much is controversial)
Take Home Points
- ACL tear is a diagnosis that can be made of physical exam. Learn multiple exam maneuvers to increase diagnostic accuracy.
- Always check for concurrent injuries to other structures in the knee such as bones and other ligaments if you suspect an acute ACL tear.
- Acute management is RICE, analgesia, and referral to orthopedics
Read More
Ortho Info: Anterior Cruciate Ligament (ACL) Injuries
Ortho Bullets: ACL Tear
Spindler KP. Clinical practice. Anterior cruciate ligament tear. N Eng J Med. 2008;359(20):2135. PMID: 19005197
References
Miyasaka, KC. The Incidence of Knee Ligament Injuries in the General Population. Am J Knee Surg. 1991; 4:43. PMC: 3037119
Agel, J. Collegiate ACL Injury Rates Across 15 Sports: National Collegiate Athletic Association Injury Surveillance System Data Update (2004-2005 Through 2012-2013). Clin J Sports Med. 2016; 26 (6):518-523. PMID: 27315457
Lelli, A. The “Lever Sign”: A New Clinical Test for the Diagnosis of Anterior Cruciate Ligament Rupture. Knee Surg Sport Trauma Arthro 2016 ;24(9):2794-7. PMID: 25536951
Boden, BP. Mechanisms of Anterior Cruciate Ligament Injury. Orthopedics. 2000;23(6):573. PMID: 10875418
Benjaminse, A. Clinical diagnosis of an anterior cruciate ligament rupture: a meta-analysis. J Ortho Sports Phys Therapy. 2006;36(5):267. PMID: 16715828
Crawford, R. Magnetic resonance imaging versus arthroscopy in the diagnosis of knee pathology, concentrating on meniscal lesions and ACL tears: a systematic review. Br Med Bull 2007;84:5-23. PMID: 17785279
Skovgaard Larsen, LP. Diagnosis of acute rupture of the anterior cruciate ligament of the knee by sonography. Eur J of Ultrasound. 2000;12(2):163. PMID: 11118925
Ardern, CL. Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery: an updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. Br J Sports Med. 2014;48(21):1543-1522. PMID: 25157180
be wary of the multiligament disruptions, they are an emergency and ofetn require repair within 10 days eg for posterolateral corners