Background
Definition: Tear of the Achilles Tendon, most frequently 4-6 cm above calcaneal tendon insertion
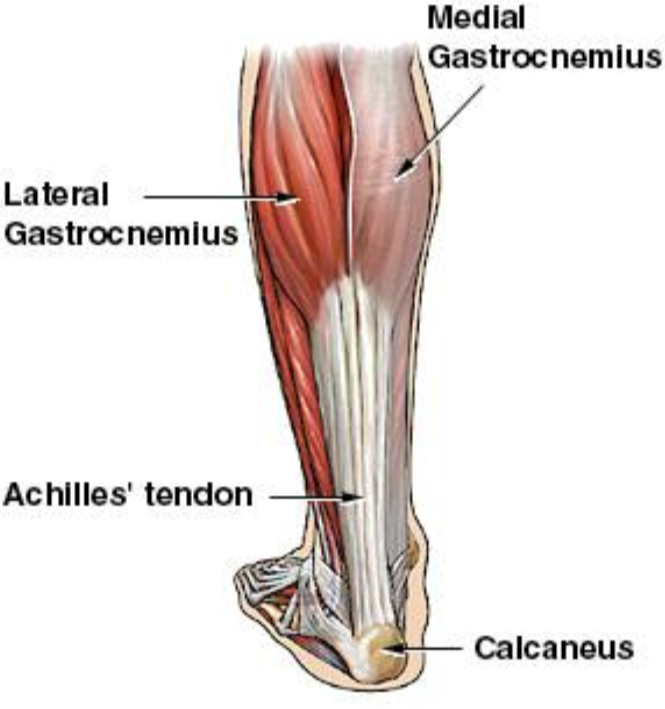
Achilles Tendon Anatomy (specialtyorthony.com)
Anatomy
- The Achilles tendon is the largest tendon in the body
- It is formed by the convergence of the soleus muscle tendon and medial and lateral gastrocnemius tendons (see figure 1 above)
- This tendon receives blood supply from posterior tibial artery
- Rupture usually occurs 4-6 cm above the calcaneal insertion in hypovascular region or “watershed/critical” zone
Mechanism
- ~80% of these injuries occur as a traumatic injury during a sporting event (Leppilahti 1998)
- May occur with
- Sudden forced plantar flexion
- Extreme dorsiflexion in a plantar flexed foot
Epidemiology
- Often misdiagnosed as an ankle sprain, and may be missed in up to 25% of cases
- Incidence 18-29:100,000 per year, and is rising (Chiodo 2006, Sheth 2017)
- Risk factors:
- Flouroquinolone antibiotics (particularly when used concomitantly with systemic steroids)
- Steroid injections
- Chronic inflammatory conditions (SLE, rheumatoid arthritis)
- Episodic athletes, also known as “weekend warriors”
- Most commonly in men aged 40-50 (Sheth 2017)
History
- Patients may state they felt a “pop”
- May have palpable gap or deformity in region of tendon

Achilles Tendon Rupture Exam (www.lfaclinic.co.uk)
Physical Exam
- Weakness with plantar flexion
- Increased resting ankle dorsiflexion on affected side in prone position with knees bent
- Palpable gap in dorsal portion of heel
- Calf atrophy in chronic cases
- Usually in absence of bony tenderness unless accompanied by other injury
- Thompson Test (video)
- Place the patient in the prone position, with feet hanging over the end of a stretcher or table. If patient is not able to lay down/there are no stretchers, the patient can kneel on a stool or chair
- Squeeze the calf of the normal limb. You will notice the squeeze will cause the ankle to plantar flex appropriately
- Squeeze the calf of the limb with the suspected Achilles tendon rupture. You will notice the squeeze will cause no motion if there is a full rupture/tear, and diminished motion if there is a partial tear
- Performance Characteristics (Garras 2012)
|
Sensitivity |
Specificity |
(+) LR |
(-) LR |
|
96-100% |
93-100% |
13.7 |
0.04 |
Imaging
- X-Rays
- Used to rule out other or concurrent pathology
- May show soft tissue swelling and destruction of pre-Achilles fat pad (Kager’s Fat Pad)
- Findings are non-specific as tear of tendon unable to be visualized
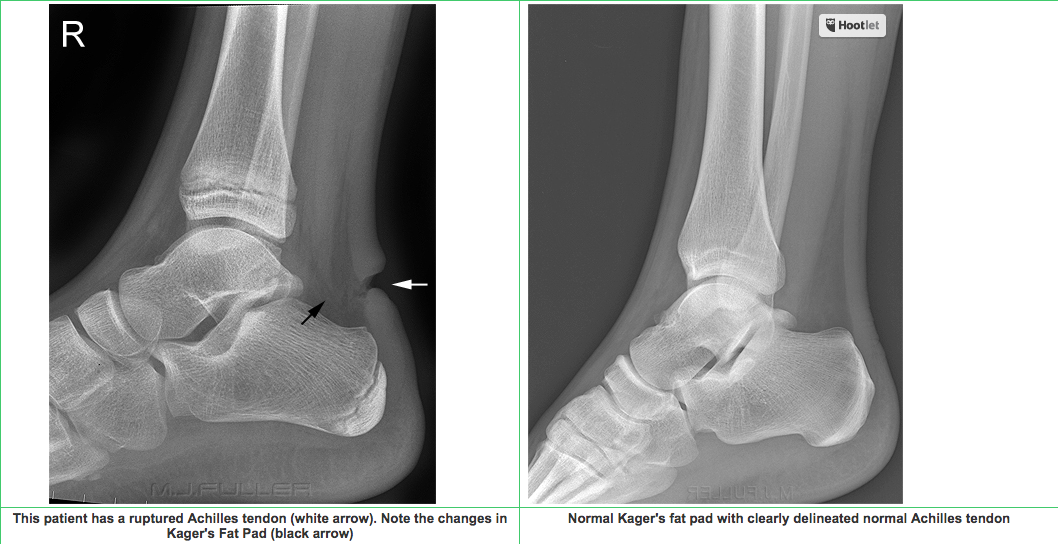
Kager’s Fat Pad (wikiradiography.net)
- Ultrasound
- Ultrasound is helpful if obvious findings present and to distinguish between partial vs complete tears, however only around 50% sensitive for detecting only partial tears (Kayser 2005)
- Normal Achilles tendon . In the image below, you can visualize the intact tendon in between the two white crosses. You will notice there is no tear or surrounding edema/fluid
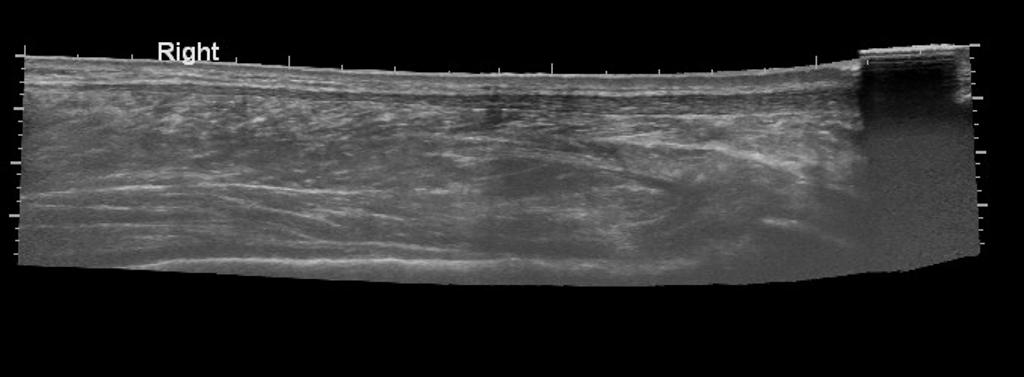
Case courtesy of Dr Maulik S Patel, Radiopaedia.org. From the case rID: 9759
- Full thickness rupture of Achilles Tendon: The retracted tendon appears to the left, with an anechoic area representing a defect full of fluid adjacent to ruptured tendon (to the right, as labeled)
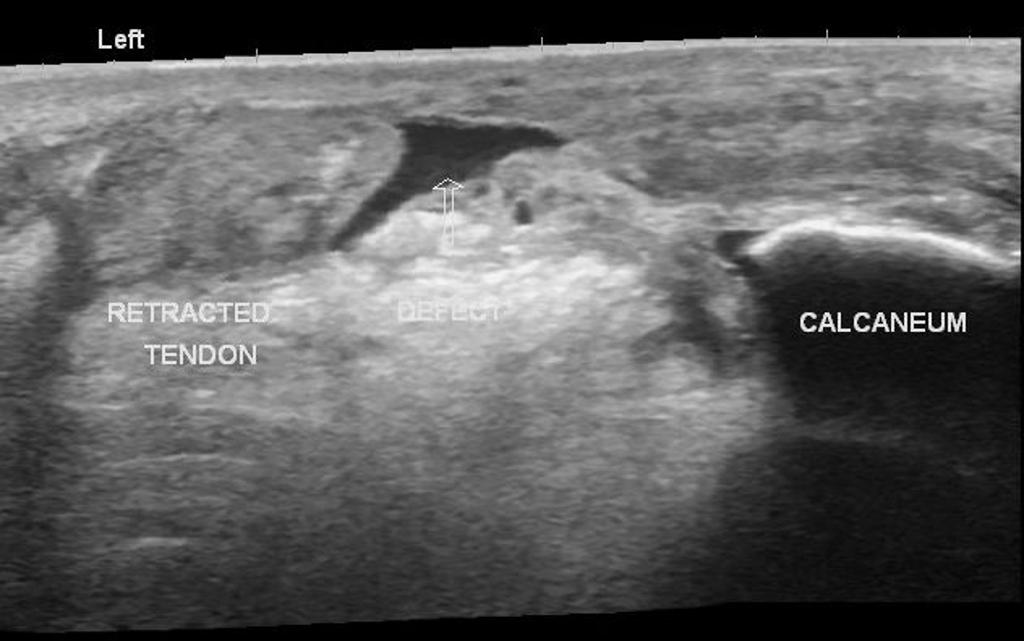
Case courtesy of Dr Maulik S Patel, Radiopaedia.org. From the case rID: 13548
- Partial thickness rupture: In the image below there is a partial thickness tear indicated in between the white arrows. Partial tears show a more hypoechoic and thickened portion of the tendon as you near the tear, as seen to the right of the midline of the image
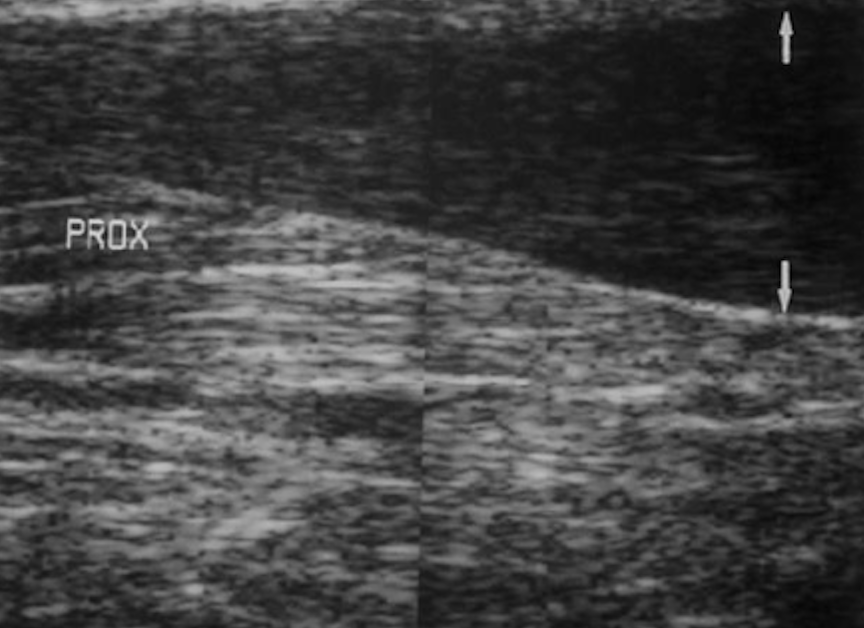
Partial Thickness Tear (orthobullets.com)
- MRI
- Gold-standard imaging modality
- Rarely, if ever, necessary in the ED
- Used for equivocal physical exam/alternate imaging findings or for assessing the severity of the tear for possible operative management
- Findings
- A full-thickness tear often shows a tendinous gap filled with edema or blood
- Complete rupture shows retraction of tendon ends

Resting Equinus Position (achillesblog.com)
ED Management
- Provide analgesia
- Tendon stabilization in an optimal healing position
- Functional bracing/splinting in resting equinus/talipus equinus
- AO splint/brace in 20 degrees of plantar flexion for 4-6 weeks (may use tall CAM boot with 20 degrees wedge inserts)
- All patients should be non-weightbearing
- Any weight-bearing can convert a partial tear to a complete tear
- Maintain non-weightbearing status until see orthopedics (within 1 week)
- After evaluation by orthopedics, early weight-bearing and early ROM exercises yield better outcomes (can be as early as 2 weeks)
- Referral to rehab warranted to improve plantar flexion and decrease risk of re-rupture
- ED Ortho consultation: patients with open wounds in the area of trauma, or with concomitant fractures
- Operative Management is usually reserved for acute ruptures (approximately <6 weeks) of full thickness with large tendon gaps, failed conservative treatment of partial thickness tears, or high performance athletes
- These cases will be determined during follow up with orthopedics and may warrant outpatient MRI to assess severity of tear
Prognosis
- For conservative management, there is no significant difference in plantar flexion strength (Willits, 2010)
- Some increased risk of re-rupture compared to operative management, although review of evidence shows that this may not be significant if patients used structured, accelerated rehab protocol.
- Protocol includes initially non-weightbearing cast with the foot in equinus position as described above, then transitioned to a pneumatic walker with elevated heels (elevation gradually reduced biweekly), and physical therapy to improve gait, strength, and mobility. (Wallace 2011)
- If addressed early and appropriately, most patients have good self-reported long-term outcomes regardless of the treatment modality
Take Home Points
- Achilles tendon rupture is a clinical diagnosis. The Thompson Test should be applied in all suspected cases
- Remember to brace or splint a rupture, even if suspected, in the resting equinus position for optimal healing and prevention of further injury
- Schedule follow up with orthopedics within 1 week for discussion of operative management vs early rehab protocols
Read More
Orthobullets: Achilles Tendon Rupture
References
Sheth U et al. The epidemiology and trends in management of acute Achilles tendon ruptures in Ontario, Canada: a population-based study of 27,607 patients. Bone Joint J. 2017; 99-B(1): 78-86. PMID: 28053261
Chiodo CP, Wilson MG. Current Concepts Review: Acute Ruptures of the Achilles Tendon. Foot Ankle Int 2006; 27(4): 305-13. PMID: 16624224
Leppilahti J, Orava S. Total Achilles tendon rupture. A review. Sports Med. 1998; 25(2): 79-100. PMID: 9519398
Kayser R et al. Partial rupture of the proximal Achilles tendon: a differential diagnostic problem in ultrasound imaging. Br J Sports Med. 2005; 39(11): 838-42. PMID: 16244194
Margetic P et al. Comparison of ultrasonographic and intraoperative findings in Achilles tendon rupture. Coll Antropol. 2007; 31:279-284. PMID: 17598414
Garras DN et al. MRI is Unnecessary for Diagnosing Acute Achilles Tendon Ruptures: Clinical Diagnostic Criteria. Clin Orthop Relat Res 2012; 470(8): 2268-2273. PMID: 22538958
Willits K et al. Operative versus nonoperative treatment of acute Achilles tendon ruptures: a multicenter randomized trial using accelerated functional rehabilitation .J Bone Joint Surg Am. 2010; 92(17): 2767-75. PMID: 21037028
Wallace RG et al. The non-operative functional management of patients with a rupture of the tendo Achillis leads to low rates of re-rupture. J Bone Joint Surg Br 2011; 93(10):1362-6. PMID: 21969435
Erickson BJ. Is Operative Treatment of Achilles Tendon Ruptures Superior to Nonoperative Treatment? Orthop J Sports Med. 2015; 3(4): PMID: 26665055
Great article! Very informative overview of Achilles tendon rupture. I appreciate the clear explanation of diagnosis and treatment options. It’s a valuable resource for both clinicians and patients. Thanks for sharing!