Definition: Sprain or tear of the acromioclavicular (AC) and coracoclavicular (CC) ligaments.
Mechanism: Typically a fall on or direct blow to the acromion with the humerus adducted, forcing the acromion inferiorly and medially relative to the clavicle.
Epidemiology
- True incidence unknown because many with mild injuries do not seek medical attention.
- Most common type of shoulder injury amongst young athletes.
- Male predominance 5:1 due to increased participation in contact sports. (Rockwood 1996)
Physical Exam

AC Joint Injury (www.shouldersurgery.com)
- Point tenderness to palpation over the AC joint and, depending on degree of injury, the CC joint.
- Prominence of the clavicle and associated swelling in more severe injuries.
- Arm typically held in adduction against the body with poor range of motion of the shoulder secondary to pain.
- Scarf test – patient elevates arm to 90 degrees and adducts across the front of the body, elicited pain in the AC joint is a positive test.
- Review of the complete shoulder exam
Injury Classification System
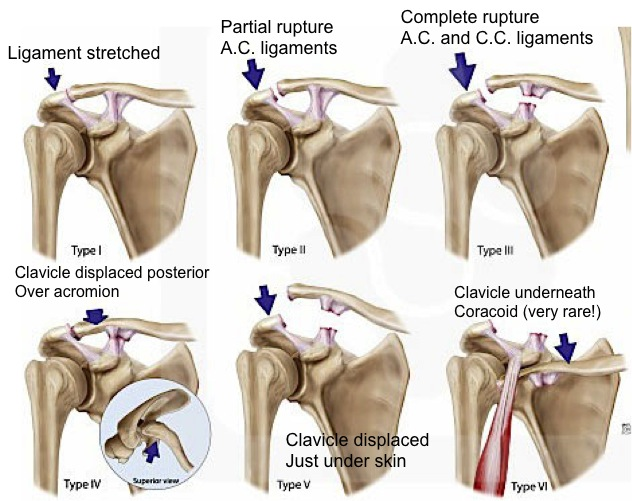
Rockwood Classification System (http://bostonshoulderinstitute.com/patient-resources/modules/ac-joint-injuries/)
- Rockwood Classification
- Type I: AC sprain, unaffected CC ligament; normal x-ray or slight AC widening.
- Type II: AC tear/CC sprain, inferior border of clavicle elevated but not displaced beyond superior aspect of acromion; normal CC space.
- Type III: AC tear/CC tear, inferior border of clavicle beyond superior aspect of acromion, CC displacement but less than twice normal joint distance.
- Type IV: AC tear/CC tear, lateral clavicle posteriorly displaced into trapezius (see on axillary view).
- Type V: AC tear/CC tear, CC displacement greater than twice normal joint distance, may cause tenting or ischemia of overlying skin.
- Type VI: AC tear/CC tear, clavicle located beneath acromion or coracoid; very rare.
X-Ray Findings
- Normal AC joint distance <5mm. Variation exists but with clinical suspicion any measurement >8mm is concerning for injury, comparison to normal contralateral side also useful.
- Normal CC joint distance 10-13mm. Displacement measured from superior border of the coracoid process to the inferior border of the clavicle.
- A Zanca view, an AP with 10-15 degrees cephalic tilt, may help better visualize the AC joint by eliminating overlying bony images when evaluating for type II injury.
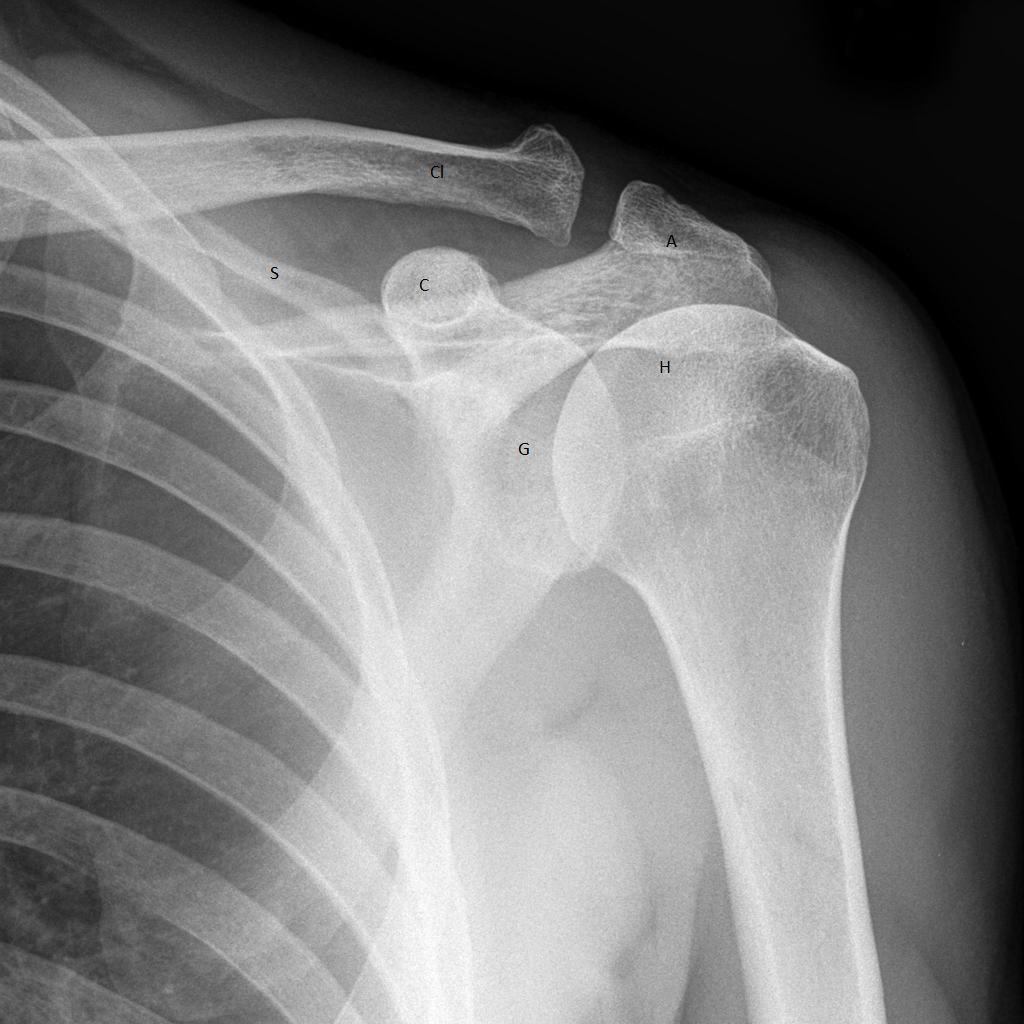
AP View of Shoulder (www.radiopaedia.org)
G – glenoid fossa
H – humeral head
A – acromion
C – coracoid process
S – scapula
Cl – clavicle
X-Ray Image Gallery

Inferior aspect of acromion and inferior distal clavicle align in normal on the left, subluxation on the right (Accident and Emergency Radiology: A Survival Guide)

Grade II AC Injury - Also seen are associated scapular and coracoid fractures.

Grade III Injury
Emergency Department Management
- Grade I and II injuries: sling for 3-7 days, taking into account severity of pain and patient age. Encourage early range of motion, especially in elderly patients. (Montellese 2004)
- Type III injuries: Ensure orthopedic follow up for possible operative management.
- Type IV-VI injuries: Uncommon and are frequently in the setting of polytrauma. They require careful examination to evaluate for signs of vascular injury. Orthopedic consultation recommended for evaluation and operative planning.
Prognosis
- Most Type I-II injuries regain full range of motion by 6 weeks and can return to normal activity by 12 weeks. Mild type I injuries may require only a few days away from usual activities.
- Type III management often dictated by patient age and lifestyle with majority being non-operative Spencer 2007. If operative management deferred patient will usually remain in a sling for 2-3 weeks.
- Return to full activity following surgery for more severe injuries is usually 6 months.
Take Home Points
- Diagnosis of AC injuries is frequently made on physical exam; lack of x-ray findings does not rule out a type I injury.
- Recommend early range of motion in commonly seen mild AC joint injuries.
- Recognize severe injury patterns and carefully evaluate for vascular compromise.
References
Baxter A. Emergency Imaging: A Practical Guide. Stuttgart, Germany: Thieme; 2016: 412-413.
Montellese P, Dancy T. The acromioclavicular joint. Prim Care. 2004; 31:857.
Quillen D et al. Acute Shoulder Injuries. Am Fam Physician. 2004; 70(10): 1947-1954. PMID: 15571061.
Raby N, Berman L, de Lacy G. Accident and Emergency Radiology: A Survival Guide. Philadelphia, PA: Elsevier Saunders; 2005: 68-89.
Rockwood CA Jr et al. Fractures in Adults. 4th ed. Philadelphia, Pa: Lippincott-Raven; 1996.
Spencer EE Jr. Treatment of grade III acrimioclavicular joint injuries: a systematic review. Clin Orthop Relat Res 2007; 455:38. PMID: 17179783.