Background: The immediate post intubation period in the ED is a critical time for continued patient stabilization. While physical adjuncts like securing the tube, in line suctioning, and elevating the head of the bed are part of general post intubation management, better understanding of analgesics and sedatives have offered newer approaches.
Early Interventions in the ED Can Have an Effect:
- The SPICE trial was a multicenter cohort study examining the hospital courses of 251 mechanically ventilated patients. Assessments of the administration of sedative agents, ventilation time and sedation depth via RASS were made. Outcomes measured included delirium and hospital plus 180 day mortality. The authors found that deep early sedation within the first four hours was an independent predictor for delayed extubation and increased mortality. (Shehabi 2012)
Analgesia:
Rapid Sequence Intubation (RSI) provides paralysis and amnesia to the patient during the process of endotracheal intubation however analgesia is typically not administered peri-procedure.
- Endotracheal tubes are painful
- A study measuring hemodynamic and respiratory variables during endotracheal suctioning showed a significant increase in RASS scores, systolic, and diastolic blood pressure in mechanically ventilated patients in patients receiving sedation only when compared to patients also receiving analgesia(Jeitziner 2012)
- Not all mechanically ventilated patients require sedatives.
- A randomized controlled trial of 140 patients compared a protocol of analgesia alone (Morphine IV bolus) versus sedation + analgesia (Propofol/Midazolam IV infusion + Morphine IV bolus). Patients in the solo analgesia group had statistically significantly more days without mechanical ventilation and on average shorter ICU length of stays. (Strom 2010)
| Analgesic | Onset | Elimination Half Life | IV Infusion Rates | Side Effects and Other Information |
| Fentanyl | 1 – 2 min | 2 – 4 hr | 0.7 – 10 μg/kg/hr | Rapid onset. Lipophilic with adipose deposition, withdrawal symptoms after prolonged infusion |
| Hydromorphone | 5 – 15 min | 2 – 3 hr | 0.5 – 3 mg/hr | No active metabolites however parent drug can accumulate in renal failure |
| Morphine | 5 – 10 min | 3 – 4 hr | 2 – 30 mg/hr | Active metabolites can accumulate in renal failure |
| Remifentanil | 1 – 3 min | 3 – 10 min | Loading dose: 1.5 μg/kg IV Maintenance dose: 0.5 – 15 μg/kg/hr |
Rapid onset. Short acting. Not affected by hepatic or renal failure. Associated with development of hyperalgesia |
| Ketamine | 30-40 sec | 2 – 3 hr | Loading dose 0.1 – 0.5 mg/kg IV followed by 0.05 – 0.4 mg/kg/hr | Attenuates the development of acute tolerance to opioids. Can cause hallucinations and other psychological disturbances. |
Adapted from Clinical Practice Guidelines for the Management ofPain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit. Critical Care Medicine 2013
Sedation:
After absence of pain is ensured, pharmacologic sedation may be indicated to help relieve discomfort, improve synchrony with mechanical ventilation and decrease oxygen requirements and overall work of breathing. (Patel 2012)
- Peri and Immediate Post Intubation Sedation
- When using a long acting paralytic (rocuronium and vecuronium), it is essential to provide a sedative and amnestic through the duration of the paralysis.
- Assessing the Sedated Patient
- Goal should be to titrate to light sedation as objectively measured by a validated scale like the Richmond Agitation-Sedation Scale (RASS)
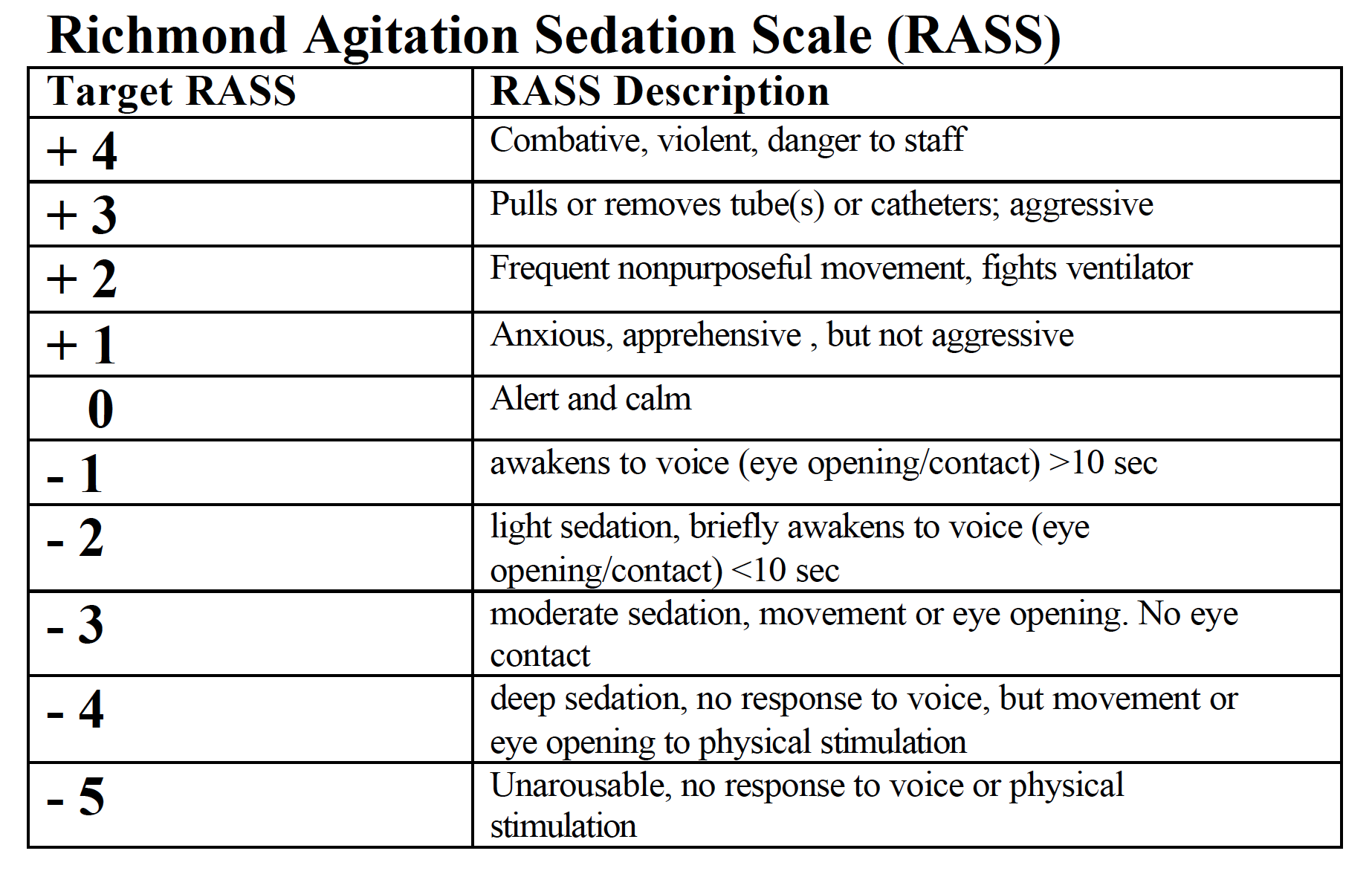
Richmond Agitation Sedation Scale (RASS) – resus.com.au
- Light Sedation > Deep Sedation
- Various studies have shown detrimental effects of prolonged deep sedation including longer mechanical ventilation times, 6 month mortality and increased incidence of delirium (Shehabi 2013)
Pharmacology of Sedative Medications
| Agent | Onset | Elimination Half Life | Loading Dose (IV) | Maintenance Dose (IV) | Side Effects and Other Information |
| Midazolam | 2 – 5 min | 3 – 11 hr | 0.01 mg – 0.05 mg/kg over several minutes | 0.02 – 0.1 mg/kg/hr | Respiratory depression, hypotension |
| Lorazepam | 15 – 20 min | 8 – 15 hr | 0.02 – 0.04 mg/kg | 0.01 – 0.1 mg/kg/hr | Respiratory depression, hypotension; nephrotoxicity |
| Diazepam | 2 – 5 min | 20 – 120 hr | 5- 10 mg | 0.03 – 0.1 mg/kg | Respiratory depression, hypotension, phlebitis |
| Propofol | 1-2 min | Short term ~ 3- 12 hr Long term ~ 50 + 18.6 hr |
5 μg/kg/min over 5 min | 5 – 50 μg/kg/min | Pain on injection, hypotension, respiratory depression, hypertriglyceridemia, pancreatitis, propofol related infusion syndrome |
| Dexmedetomidine | 5 – 10 min | 1.8 – 3.1 hr | 1 μg/kg over 10 min | 0.2 – 0.7 μg/kg/hr | Bradycardia hypotension, loss of airway reflexes |
Adapted from Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit. Critical Care Medicine 2013
Take Home Points
- Employ an analgesic-first approach to post intubation pharmacologic management
- If sedation is needed, utilize light sedation and titrate up as needed
- When using a long acting paralytic, ensure sedation and amnesia for the duration of paralysis
References
Barr J, Gilles L, Puntillo K, et al: Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit. Critical Care Medicine 2013; 41: 263-295 PMID: 23269131
Jeitziner MM, Schwendimann R, Hamers JP, et al: Assessment of pain in sedated and mechanically ventilated patients: An observational study. Acta Anaesthesiol Scand 2012; 56: 645-654 PMID: 22404146
Patel S, Kress J: Sedation and Analgesia in the Mechanically Ventilated Patient: Am J Respir Crit Care Med 2012; 185: 486-497 PMID: 22016443
Shehabi Y, Bellomo R, Reade M, et al: Early Intensive Care Sedation Predicts Long-Term Mortality in Ventilated Critically Ill Patients. Am J Respir Crit Care Med 2012; 186: 724-731 PMID: 22859526
Shehabi Y, Chan L, Kadiman S, et al: Sedation Practice in Intensive Care Evaluation (SPICE) Study Group investigators: Sedation depth and long-term mortality in mechanically ventilated critically ill adults: A prospective longitudinal multicenter cohort study. Intensive Care Med 2013; 39: 910-918 PMID: 23344834
Strom T, Martinussen T, Toft P: A protocol of no sedation for critically ill patients receiving mechanical ventilation: a randomized trial. The Lancet 2010; 375: 475-480 PMID: 20116842
