Definition: The lunate is disarticulated and, most commonly, displaced volarly from both the capitate as well as the radius.
 Mechanism:
Mechanism:
- The classic scenario involves fall on outstretched hand causing high velocity forced hyperextension and ulnar deviation of the wrist
Epidemiology:
- Carpal injuries compose 2.5% of all encounters in the ED
- Perilunate/lunate dislocations compose about 10% of carpal injuries (Perron 2001)
- 25% of perilunate/lunate dislocations are missed on initial presentation (Karadsheh 2014)
Physical Exam:
- Patients will often be tender and swollen in the volar aspect of the wrist but physical exam is unlikely to be diagnostic.
- Important to perform and document an comprehensive neurovascular exam on injured limb as volar displacement of lunate can cause compression of median nerve in the carpal tunnel.
- For systematic review of hand and wrist exam: Orthobullets: Physical Exam of the Hand
X-ray Findings:
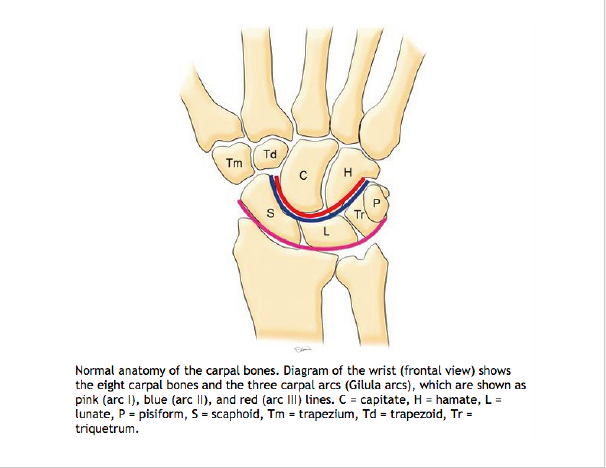
- On PA view of wrist evaluate the 3 carpal arcs known as Gilula’s arcs. Normally, the arcs should be smooth running parallel to each other.
- Arc I, most proximal and largest arc, include the proximal surfaces of the scaphoid, lunate, triquetrum and pisiform
- Arc II spans the distal articular surfaces the formerly mentioned carpals.
- Arc III include the proximal surfaces of the capitate and hamate.
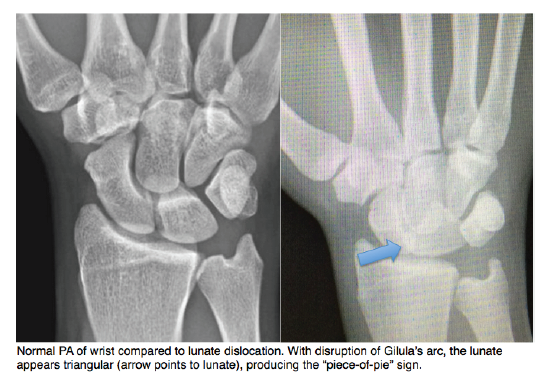
- In lunate dislocations, disruption of Gilula’s arcs can be appreciated with disruption of spaces between the proximal and distal carpal bones. The lunate is rotated forming a triangular shape commonly known as the “piece-of-pie” sign.
- On lateral view of the wrist evaluate for the alignment of the 4Cs or the articulations of the lunate with the radius
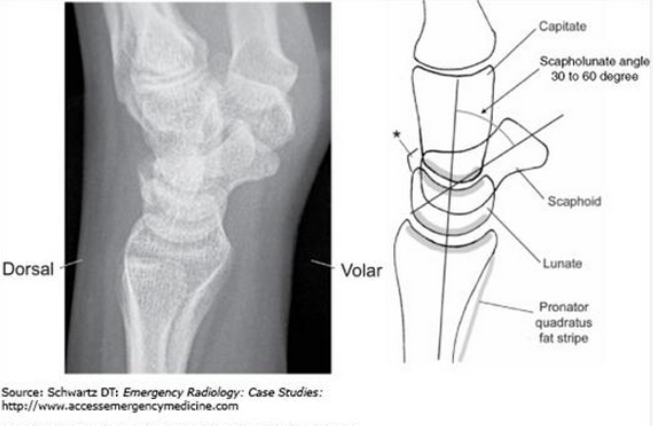
proximally and the capitate distally.- The proximal 2 Cs indicates the articulation between the lunate and the radius
- The distal 2 Cs indicates the articulation between the lunate and capitate.
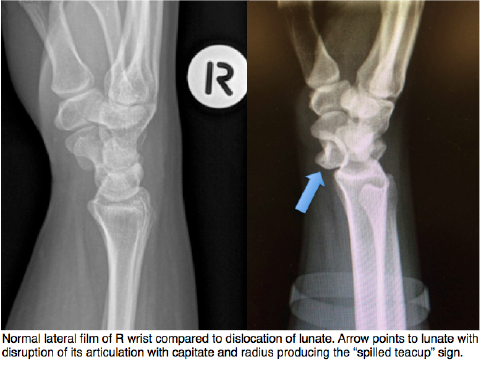
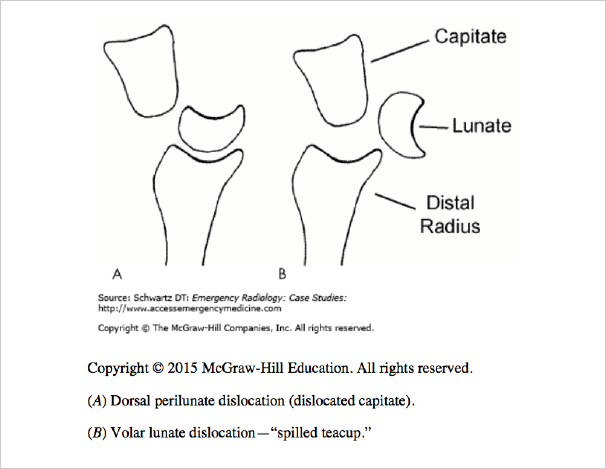
- In lunate dislocations, the lunate’s articulations with both the radius and capitate are disrupted displacing the lunate volarly creating a “spilled teacup”
Classification: The Mayfield classification derived from cadaveric studies on pathoanatomy of carpal ligamentous injury is the most well recognized classification of carpal injuries organized into 4 stages (Karadsheh 2014, Perron 2001).
- Stage I- Scapholunate dislocation noted on PA of wrist film with increased space between scaphoid and lunate
- Stage II & III –Perilunate dislocations
- Stage IV-Lunate dislocation
- The main differentiating factor between perilunate and lunate dislocation is the lunate’s articulation with the radius. In perilunate dislocations, the lunate’s articulation with the radius is preserved with the capitate dorsally displaced whereas in lunate dislocations, the lunate is disarticulated from both the capitated as well as the radius (Schwartz 2008).
ED Management:
- Immediate closed reduction and splinting should take place with early operative referral
- General steps of closed reduction include traction followed by wrist extension, more traction, wrist flexion with volar pressure applied to rearticulate the lunate with the radius
- Video of closed perilunate/lunate reduction: Lunate or Perilunate Dislocation?
- Some argue that immediate operative treatment of perilunate/lunate dislocations result in better functional outcome, but this has not been adopted as standard care (Kannikeswaran 2010)
Prognosis:
- No prognostic difference between perilunate and lunate dislocations (Kannikeswaran 2010)
- Untreated or delayed treatment leads to poor functional outcomes. Chronic and progressive arthritis, decreased range of motion, joint dysfunction and disability are common. (Escarza 2011, Perron 2001)
Take Home Points:
- Suspect lunate dislocations in any patient with an appropriate mechanism of injury (FOOSH) and tenderness of the wrist.
- On PA X-ray of the wrist, evaluate Gilula’s arcs; look for “piece of pie” sign
- On lateral X-ray of the wrist, evaluate the 4 C’s; look for “spilled teacup” sign
- All lunate dislocations should be emergently reduced and referred for early orthopedic assessment for surgery.
References:
Escarza R et al. Chapter 266. Wrist injuries. In: Tintinalli JE, Stapczynski J, Ma O, Cline DM, Cydulka RK, Meckler GD, T. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7e. New York, NY: McGraw-Hill; 2011.
Kannikeswaran N, Sethuraman U. Lunate and perilunate dislocations. Pediatr Emerg Care. 2010; 26(12):921-4. PMID: 21131804
Karadsheh M. Lunate Dislocation (Perilunate dissociation). (2012, December 24) [Ortho Bullets] Retrieved from: http://www.orthobullets.com/hand/6045/lunate-dislocation-perilunate-dissociation.
Kastelec M et al. Carpus – Complete dislocation of the lunate. [AO Foundation] Retrieved from http://bit.ly/1Jsrftz.
Perron AD et al. Orthopedic Pitfalls in the ED: Lunate and perilunate injuries, Am J Emerg Med 2001; 19(2):157-62. PMID: 11239263
Schwartz DT. Perilunate Injuries. In: Schwartz DT. eds. Emergency Radiology: Case Studies. New York, NY: McGraw-Hill.
