Author: Erica Cohen, MD
Editor: Ellen Duncan, MD, PHD
Introduction
- Measles is a highly contagious viral illness caused by the rubeola virus. It spreads via airborne transmission and can remain infectious on surfaces or in the air for up to 2 hours.
- The infectious period begins 4 days before the rash onset, leading to frequent misdiagnosis as a nonspecific viral infection during the prodromal period.
- Though measles was eradicated in the U.S. in 2000, outbreaks persist in areas with low vaccination rates.
- In 2024, global measles vaccination rates (84%) remained below the ~95% threshold for herd immunity; in that year, measles caused 11 million infections and 95,000 deaths globally.
- In the US in 2025, there were 49 outbreaks and 2,144 confirmed cases of measles
- High-risk populations: infants, pregnant individuals, and immunocompromised patients.
Clinical Manifestations
- Measles progresses through 4 stages:
- Incubation period (7–14 days): Typically asymptomatic
- Prodromal stage (2–4 days):
- High fever (≥ 102°F–104°F)
- “3 C’s” Triad: Cough, coryza, conjunctivitis
- Koplik spots: Pathognomonic tiny white lesions on buccal mucosa
- Exanthem stage: Blanching maculopapular (morbilliform, or “measles-like”) rash, spreading cephalocaudally. Rash darkens and may desquamate.
- Recovery: Symptoms fade in reverse order.
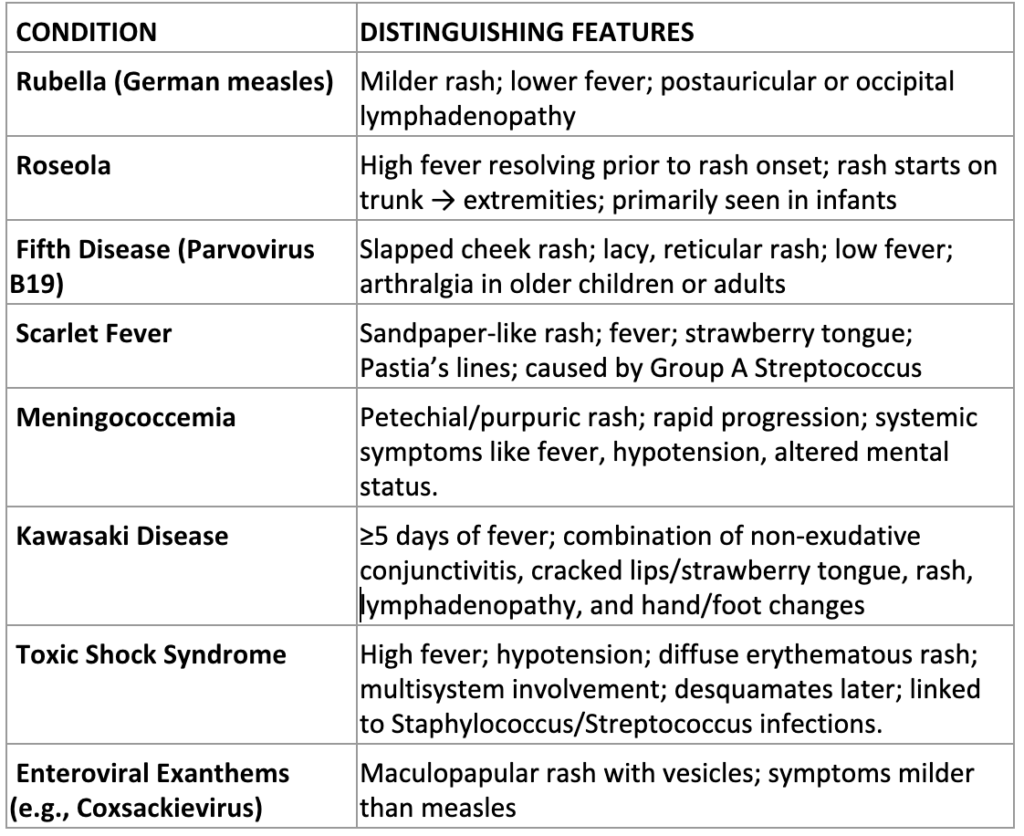
Differential Diagnosis
Complications
- ~30% of patients develop complications and 25% require hospitalization. High-risk groups include children <5 years, immunocompromised and pregnant patients, adults, and people with malnutrition and/or vitamin A deficiency.
- Common complications include otitis media and diarrhea.
- Severe non-neurologic complications include pneumonia, croup, severe dehydration.
- Neurologic complications include:
- Encephalitis: ~1 in 1,000 patients, typically within 5 days of rash onset
- Acute disseminated encephalomyelitis: ~1 in 1,000; autoimmune reaction during recovery phase.
- Subacute sclerosing panencephalitis: 4–11 per 100,000; fatal CNS disease seen years later, particularly in infants
- Post-measles immune amnesia and immunosuppression can persist for weeks to months, increasing risk for secondary infections
Testing
- Key tests include basic bloodwork, serum IgM/IgG antibodies and measles-specific PCR from blood, throat, nasopharynx, or urine
- IgM may be falsely negative if obtained within the first 72 hours of rash onset and should be repeated if suspicion remains high
- CXR (evaluate pneumonia/interstitial pneumonitis).
- Measles is immediately reportable; reporting is critical for contact tracing and outbreak control.
Treatment and Isolation
- Supportive care: Hydration, antipyretics, management of complications.
- Vitamin A supplementation has been shown to reduce severity/mortality; dosing below:
- <6 months: 50,000 IU PO daily × 2 days.
- 6–11 months: 100,000 IU PO daily × 2 days.
- ≥12 months: 200,000 IU PO daily × 2 days.
- Severe cases: Third dose 2–4 weeks later.
- Ribavirin can be considered but is not FDA-approved for measles treatment.
- Patients are infectious from 4 days before through 4 days after rash onset, and airborne precautions and a negative-pressure room should be used throughout this time. Immunocompromised patients may be infectious for longer and should remain on airborne precautions throughout the duration of illness.
Disposition
- Patients with the following should be admitted to the hospital: severe dehydration, respiratory compromise, or neurologic involvement; patients < 12 months; pregnant or immunocompromised patients.
- Clinically stable children without high-risk features may be managed outpatient with strict isolation and return precautions.
Vaccination and Post-Exposure Prophylaxis (PEP)
- MMR vaccine: routine childhood administration at 12 months and 4 years (93% effective after 1 dose, 97% after 2 doses).
- Early doses (6–12 months) recommended during outbreaks or for high-risk international travel.
- Post-exposure prophylaxis:
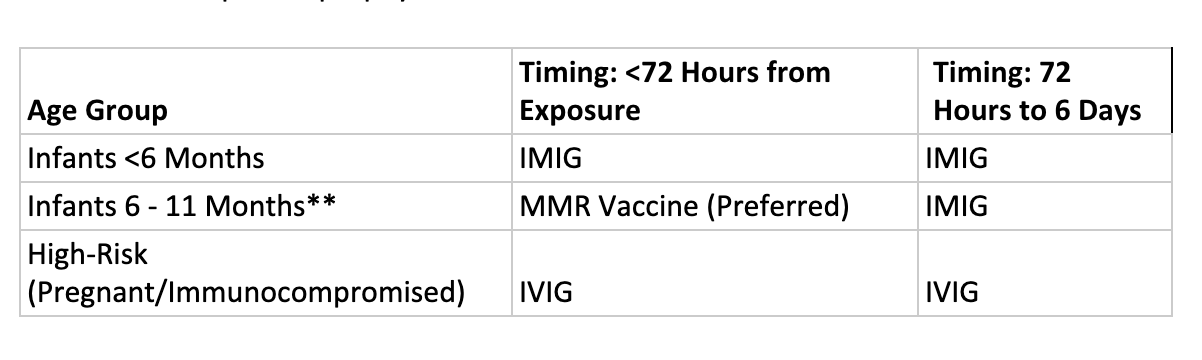
- Of note: Pregnant or severely immunocompromised patients should not receive the vaccine.
- ** Infants <12 months of age are at higher risk for (1) complications and (2) severe measles, and are at increased risk of infection if (1) the mother is not immune or (2) lacks maternal antibodies. Thus, IMIG should be given to any infant <12 months of age with a known exposure to measles. However, any infant between 6-11 months may receive the MMR vaccine in place of IMIG IF administered within 72 hours of exposure (CDC Prevention of MMR).
Summary
- Measles is a highly contagious viral illness with cough, coryza, conjunctivitis, fever, and cephalocaudal maculopapular rash.
- Diagnosis: clinical recognition, confirm with IgM and PCR.
- Management: supportive care, vitamin A, airborne isolation, public health reporting.
- Prevention: vaccination is key; post-exposure prophylaxis available.
- Centers for Disease Control and Prevention. Measles data and statistics. Centers for Disease Control and Prevention website.
https://www.cdc.gov/measles/data-research/index.html - World Health Organization. Measles: fact sheet. World Health Organization website.
https://www.who.int/news-room/fact-sheets/detail/measles - Centers for Disease Control and Prevention. Prevention of measles, mumps, and rubella: recommendations of the Advisory Committee on Immunization Practices (ACIP). Centers for Disease Control and Prevention website.
https://www.cdc.gov/mmwr/preview/mmwrhtml/rr6204a1.htm