Authors:
Jonathan Kobles, MD and Matthew Generoso, MD
Case:
- A 25-year-old female with no significant past medical history presents to the Emergency Department with right jaw pain and inability to close her mouth. She reports an episode of nausea and stomach cramping and a sensation that she was about to vomit. After running to the bathroom and attempting to vomit, she felt a clicking sensation in her jaw (worse on the right side) and afterward was unable to close her mouth. She states this has never happened to her before, and she denied any direct trauma to her face, jaw, or mouth.
- On exam, her mouth is held open and she is unable to fully close her mouth. She has no significant facial swelling, and no evidence of intraoral trauma. She has mild tenderness to her right temporomandibular joint (TMJ), where she is suspected to have an anterior TMJ dislocation.
- She is given 30 mg of intramuscular ketorolac and 5 mg of intramuscular diazepam.
- Reduction of her anterior TMJ dislocation is attempted with both extra-oral and intra-oral manipulation, without success and with significant discomfort from the patient.
Background:
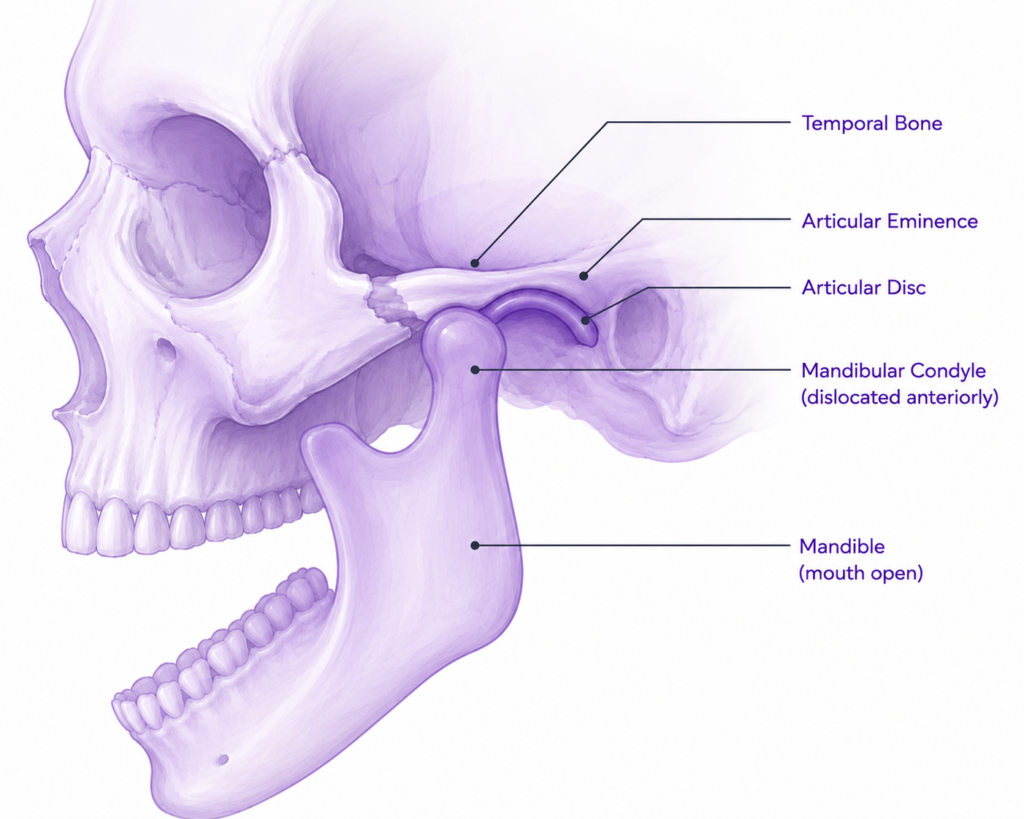
- Temporomandibular joint (TMJ) dislocation occurs when the mandibular condyle becomes trapped anterior to the articular eminence, preventing spontaneous reduction and leaving the patient unable to close their mouth.
- Most ED presentations involve acute anterior dislocations following routine activities that require excessive mouth opening, including yawning, laughing, vomiting, singing, dental procedures, or endoscopy.
- Traditional reduction methods rely on provider-applied force and may require procedural sedation. The syringe technique offers a patient-driven alternative that can often be performed without sedation and may be particularly useful in patients with recurrent atraumatic dislocations.
Epidemiology
- Anterior dislocations account for the overwhelming majority of TMJ dislocations encountered in clinical practice. Bilateral dislocations occur more commonly than unilateral dislocations and are frequently associated with atraumatic mechanisms.
- Patients at highest risk for recurrence include those with prior dislocations, generalized ligamentous laxity, connective tissue disorders, abnormal joint anatomy, and neuromuscular conditions that alter normal jaw mechanics.
- Recurrent dislocators represent the population most likely to benefit from learning the syringe technique as a future self-reduction maneuver.
Clinical Presentation:
- Patients typically present with an inability to close their mouth accompanied by preauricular pain, difficulty speaking, excessive salivation, and inability to chew normally.
- On examination, the jaw is fixed in an open position. Bilateral dislocations generally produce a symmetric appearance, whereas unilateral dislocations often cause deviation of the mandible toward the unaffected side.
- The diagnosis is usually clinical. Imaging should be reserved for patients with significant trauma, concern for fracture, atypical findings, or failed reduction attempts.
Differential Diagnosis:
- Mandibular fractures, particularly condylar fractures, should be considered in patients with traumatic mechanisms, persistent malocclusion, facial deformity, or focal bony tenderness.
- Deep neck space infections, peritonsillar abscesses, and epiglottitis may mimic TMJ dislocation by causing drooling, muffled speech, and difficulty handling secretions, though associated infectious symptoms are typically present.
- TMJ internal derangement, acute dystonic reactions, and tetanus can all produce abnormal jaw positioning or restricted jaw movement and should be considered when the clinical presentation is atypical.
The Syringe Technique:
Patient Selection
- Ideal candidates are awake, cooperative patients with an acute atraumatic anterior dislocation and no evidence of associated fracture.
- The technique should generally be avoided in patients with significant facial trauma, altered mental status, inability to cooperate, or concern for mandibular fracture.
Procedure
- Place a 5- or 10-mL syringe between the upper and lower posterior molars on the affected side.
- Instruct the patient to bite gently and slowly roll the syringe back and forth.
- Continue until reduction occurs.
- If the initial attempt is unsuccessful, repeat the maneuver on the contralateral side.


Mechanism
- Rolling the syringe creates gradual rotational movement of the mandible while promoting relaxation of the muscles of mastication. As muscular tension decreases, the condyle is able to traverse the articular eminence and return to its normal position.
Advantages
- The clinician’s fingers never enter the patient’s mouth, little force is required, procedural sedation can often be avoided, and the technique can frequently be completed within minutes using readily available equipment.
Self-Reduction
- Unlike traditional reduction techniques, the syringe method places the reduction force in the hands of the patient. For carefully selected individuals with recurrent atraumatic dislocations, the maneuver can be taught as a potential self-management strategy to reduce future need for emergency department visits.
Evidence:
- In the original prospective case series by Gorchynski and colleagues, 30 of 31 patients experienced successful reduction using the syringe technique, corresponding to an approximately 97% success rate.
- Most reductions occurred rapidly and did not require procedural sedation, supporting the technique as an effective first-line option for uncomplicated anterior dislocations.
Traditional Reduction Techniques:
Although the syringe technique is increasingly popular, several established reduction methods remain widely used in Emergency Medicine. These techniques can be divided into intra-oral and extra-oral approaches.
Intra-oral Techniques
Bimanual Reduction
- The provider places both thumbs on the lower molars while wrapping the remaining fingers around the mandible. Downward pressure is applied to disengage the condyle, followed by posterior guidance back into the glenoid fossa.
- This remains the most commonly taught reduction technique but often requires significant force, patient relaxation, and occasionally procedural sedation.
Wrist Pivot Technique
- The provider places their fingers on the lower molars and thumbs beneath the chin. A rotational wrist motion elevates the chin while simultaneously depressing the posterior mandible, facilitating reduction.
- Compared with the classic technique, the wrist pivot method may require less force and can be ergonomically advantageous for the operator.
Supine Technique
- The patient lies supine while the provider stands behind the head of the bed and performs a reduction maneuver similar to the classic method.
- Positioning allows the provider to use body mechanics rather than arm strength and may improve procedural comfort.
Extra-oral Techniques
External Reduction Technique
- The provider manipulates the mandible entirely from outside the mouth by applying simultaneous pressure to the mandibular angle and coronoid region.
- This avoids placing fingers between the patient’s teeth and eliminates the risk of bite injury.
Choosing a Technique
- No single reduction method is clearly superior for all patients.
- Traditional intra-oral techniques remain effective but may require greater force, analgesia, or sedation.
- Extra-oral approaches reduce provider exposure to bite injury and may improve patient tolerance.
- For uncomplicated atraumatic anterior dislocations, the syringe technique represents a simple first-line option because it is rapid, inexpensive, and patient-driven.
Prognosis and Complications:
- Outcomes following successful reduction of an isolated anterior TMJ dislocation are excellent, with most patients experiencing immediate symptom resolution and discharge from the Emergency Department.
- Recurrence remains the most important long-term complication. Repeated dislocations may contribute to progressive capsular laxity, chronic instability, and degenerative changes within the joint.
- Serious complications are uncommon but can include mandibular fracture, condylar injury, ligamentous damage, neurovascular injury, and complications related to traumatic posterior or superior dislocations.
Return to the Case:
- After attempting both extra-oral and intra-oral manual manipulation of her TMJ dislocation, the syringe technique is attempted.
- The patient first places a 10mL syringe between her upper and lower molars on the left side of her face (contralateral to her likely dislocation) and rolls the syringe between her teeth.
- Immediately after placing the syringe between her teeth on the left, she feels a “clunk” in her right TMJ region, is able to fully close her mouth and elevate her mandible, and begins to feel resolution of her pain.
- The patient’s TMJ remains reduced for the rest of her Emergency Department stay, and is discharged without need for further reduction attempts or imaging.
Take Home Points:
- Most ED TMJ dislocations are anterior and atraumatic.
- The syringe technique is a simple, sedation-sparing reduction strategy with a high reported success rate.
- Recurrent dislocators are ideal candidates for this approach.
- The technique can potentially be taught as a future self-reduction maneuver.
- A simple syringe may help selected patients avoid repeat Emergency Department visits.
References:
- Gorchynski J, Karabidian E, Sanchez M. The “syringe” technique: a hands-free approach for the reduction of acute nontraumatic temporomandibular dislocations in the emergency department. J Emerg Med. 2014;47(6):676-681. doi:10.1016/j.jemermed.2014.06.050.
- Hillam J, Isom B. Mandible Dislocation. In: StatPearls. Treasure Island (FL): StatPearls Publishing; Updated July 24, 2023. Available from: NCBI Bookshelf.
- Liddell A, Perez DE. Temporomandibular joint dislocation. Oral Maxillofac Surg Clin North Am. 2015;27(1):125-136. doi:10.1016/j.coms.2014.09.005.
- Prechel U, Ottl P, Ahlers OM, Neff A. The treatment of temporomandibular joint dislocation. Dtsch Arztebl Int. 2018;115(5):59-64. doi:10.3238/arztebl.2018.0059.
- Sharma NK, Singh AK, Pandey A, Verma V, Singh S. Temporomandibular joint dislocation. Natl J Maxillofac Surg. 2015;6(1):16-20. doi:10.4103/0975-5950.168222.
