Author: Cooper Urban MS4
Editor: Jackie Gomberg, MD
Overview:
Scrotal, or testicular, ultrasound is a rapid bedside tool that can be used to evaluate acute testicular complaints and identify emergencies requiring urgent intervention.
This review will focus on using ultrasound as a diagnostic tool in the following conditions:
- Testicular Trauma
- Acute Testicular Pain
- Painless Testicular Swelling
Indications:
Indications for testicular ultrasound in the emergency department include but are not limited to:
- Testicular pain
- Trauma
- Testicular asymmetry / swelling
- Palpable testicular mass
Contraindications:
There are no absolute contraindications to testicular ultrasound.
Technique:
- Begin with the patient in the supine position, with a sheet or cloth placed on the patient’s thighs to support and elevate the scrotum. The penis is positioned superolaterally and covered.
- The high-frequency (8-15MHz), linear array probe is used for enhanced resolution of superficial structures.
- A transverse view of both testes, or a “buddy view”, should be the first image obtained to compare the symmetry, vascularity, and echogenicity of both structures.
- Spectral, power, and color Doppler settings can be used to evaluate for any asymmetry in vascularity.
Normal Anatomy:

Normal anatomy. Source: Delgado-Muñoz et al., 2021.

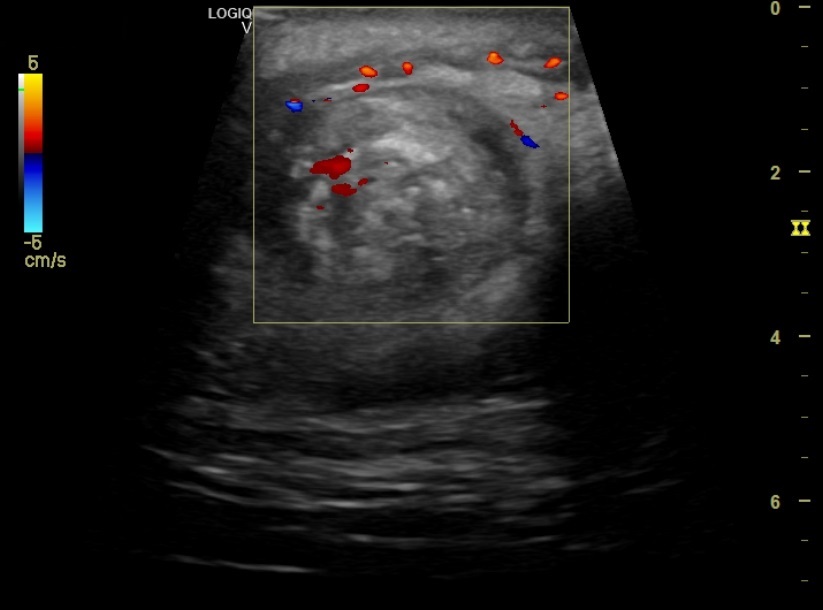
Normal color Doppler view of right testis. Source: Nikolic et al., 2012
Ultrasound Differential for Trauma:
- Testicular rupture
- Presentation: Immediate pain, swelling, nausea, and vomiting following scrotal trauma.
- Findings: Ultrasound shows discontinuity of the tunica albuginea, heterogeneous echotexture, and extrusion of testicular contents, often with associated hematocele or hemorrhage.
- Sensitivity: 100%; Specificity: 93.5% (Buckley & McAninch, 2006)
- Management: Urgent surgical exploration and repair.

Testicular Rupture. Source: Blok et al., 2019
- Intratesticular hematoma (ITH)
- Presentation: Swollen, tender testicle with visible discoloration or bruising after scrotal trauma.
- Findings: Well-defined, hypoechoic or heterogeneous intratesticular lesion with no internal flow and intact tunica albuginea. Testicular vascularity is preserved.
- Sensitivity: 71%; Specificity: 77% (Guichard et al., 2008)
- Management: Many ITHs can be managed conservatively. However, if concern for expanding hematoma or severe pain, surgical exploration may be warranted.

Intratesticular Hematoma (indicated by blue arrow). Source: Bowen & Gonzalez, 2014.
- Hematocele
- Presentation: Scrotal pain, swelling, along with a palpable lump following trauma.
- Note: While isolated hematoceles can be found following scrotal trauma, they can also be associated with more severe traumatic pathologies such as testicular rupture, fracture, or epididymal injuries.
- Findings: Complex fluid between the tunica albuginea and tunica vaginalis. Echogenic when acute, with septations or loculations as it evolves and becomes subacute or chronic.
- Sensitivity: 87%; Specificity 89% (Guichard et al., 2008)
- Management: Isolated hematoceles can be conservatively managed. However, if a more severe underlying traumatic pathology is suspected, surgical exploration may be necessary.

Hematocele – complex, septated fluid collection on longitudinal view of right hemiscrotum two weeks after a straddle injury. Source: Fenton et al., 2016.
Ultrasound Differential for Acute Testicular Pain:
- Testicular torsion
- Presentation: Abrupt onset of unilateral testicular or groin pain, typically accompanied by nausea, vomiting, and absent cremasteric reflex on the affected side.
- Findings: Absent or reduced blood flow with testicular enlargement and hypoechoic, heterogeneous echotexture. Comparison with the contralateral testis is essential.
- The presence of a twisted or spiral configuration of the spermatic cord on ultrasound, often called the whirlpool sign, strongly indicates testicular torsion.
- Note: Resistive Index (RI) is a Doppler measurement that reflects resistance to blood flow within the testicular artery and can aid in diagnosing torsion. An RI > 0.7 may indicate partial torsion, with higher values suggesting more severe loss of perfusion.
- Sensitivity: 95%; Specificity: 98% (Ota et al., 2019)
- Management: Urgent urological intervention for detorsion and orchiopexy.
- Patient’s with a high suspicion for testicular torsion or intermittent torsion should have urology consultation prior to imaging.
- In cases of intermittent torsion, ultrasound may show normal blood flow. Clinical suspicion should guide management even if imaging is inconclusive.

Testicular torsion. Source: Nakayama et al., 2020
“Whirlpool” or “Swirl” Sign. Elfeky M, Testicular trosion. Case study, Radiopaedia.org. https://doi.org/10.53347/rID-75928
- Inguinal hernia
- Presentation: An inguinal hernia can present as a bulge in the scrotum that enlarges when straining or coughing. Pain and erythema can raise concern for strangulation.
- Findings: Scrotal hernia appears as bowel or omentum within the scrotum. Peristalsis and flow suggest viability, while dilated, akinetic bowel indicates possible strangulation.
- Sensitivity: 90%; Specificity: 93% (Blaivas & Brannam, 2004)
- Management: Non-incarcerated hernias are managed conservatively with possible elective surgery, while incarcerated hernias with concern for strangulation require urgent surgical intervention.

Two loops of bowel (B) with fecal matter (F) in the scrotum. Source: Blaivas & Brannam, 2004.
- Epididymo-orchitis
- Presentation: Gradual onset of warm, painful, and swollen scrotum, accompanied by urinary symptoms.
- Findings: In epididymitis, there is typically enlargement of the epididymal head on ultrasound. If there is accompanying orchitis, Doppler will show asymmetrically increased color flow in the affected testis.
- Sensitivity: 78.8%; Specificity: 98.1% (Zitek et al., 2020)
- Management: Typically a combination of antibiotics, analgesics, and supportive management.
- Recommended Antibiotic Regimen in Epididymo-orchitis
| Patient Group | Suggested Empiric Therapy |
|---|---|
| <35 yrs, STI likely | Ceftriaxone IM once + Doxycycline 100 mg BID × 10 days |
| Insertive anal sex, STI + enteric | Ceftriaxone IM once + Levofloxacin 500 mg daily × 10 days |
| >35 yrs, likely enteric pathogens | Levofloxacin 500 mg daily × 10 days (or Ofloxacin BID) |
| Fluoroquinolone contraindicated | Amoxicillin-clavulanate TID × 10 days |

Epididymitis, shown by enlargement of the epididymal head (E). Source: Blaivas & Brannam, 2004.

Epididymo-orchitis. Normal right testis (A), with left testis (B) showing epididymis (thick arrow), increased blood flow, and reactive hydrocele (thin arrow). Source: Mandava et al., 2020.
Ultrasound Differential for Painless Swelling:
- Hydrocele
- Presentation: Painless scrotal swelling, and positive transillumination test on physical exam.
- Findings: A hydrocele appears as an anechoic fluid collection between the parietal and visceral layers of the tunica vaginalis, and can contain low-level echogenic foci if proteinaceous or infected.
- Note: Hydroceles are either primary, due to incomplete closure of the processus vaginalis, or secondary, caused by infection, trauma, or malignancy.
- Management: Typically self-resolving, so treatment is rarely necessary unless secondary to another pathology.

Hydrocele – anechoic fluid (F) surrounding testis (T).
- Spermatocele
- Presentation: Often the same as hydroceles, with painless swelling and positive transillumination.
- Findings: Spermatoceles appear as well-defined, anechoic or hypoechoic lesions typically located in the head of the epididymis.
- Note: On ultrasound, spermatoceles can demonstrate a “falling snow sign”, which describes the low-level echoes seen within the cystic fluid.
- Management: Typically self-resolving.

Spermatocele – a well-defined cystic structure within the epididymis, with fine echogenic foci (“falling snow”). Source: Radiopaedia.
- Tumor
- Note: Several tumor types can present as scrotal masses, the most common of which being seminomas.
- Presentation: Painless testicular lump
- Findings: Seminomas usually appear as homogeneous, hypoechoic masses with smooth borders. Non-seminomatous tumors are heterogeneous with ill-defined margins, cystic areas, or calcifications.
- Sensitivity: Seminoma: 76.8%; Nonseminoma: 57.7%
- Specificity: Seminoma: 84.6%; Nonseminoma: 96.4%

Seminoma – hypoechoic lesion outlined by yellow markers. Source: Hwang & Alexander, 2023.
Take Home Points:
- Testicular ultrasound is a first-line imaging modality to evaluate for scrotal pain, swelling, or traumatic injury.
- It is low-risk and offers a high degree of sensitivity and specificity for many conditions.
- As many pathologies are unilateral in nature, it is critical to compare the echogenicity, vascularity, and dimensions of both testes.
- Use color Doppler to assess blood flow.
- Ultrasound is useful to quickly evaluate for emergent diagnoses, such as testicular torsion, rupture, and incarcerated inguinal hernias.
References:
- Blaivas, M., & Brannam, L. (2004). Testicular ultrasound. Emergency Medicine Clinics, 22(3), 723-748.
- Blok, D., Flannigan, M., & Jones, J. (2019). Testicular Rupture Following Blunt Scrotal Trauma. Case Reports in Emergency Medicine, 2019. https://doi.org/10.1155/2019/7058728
- Bowen, D. K., & Gonzalez, C. M. (2014). Intratesticular hematoma after blunt scrotal trauma: A case series and algorithm-based approach to management. Central European Journal of Urology, 67(4). https://doi.org/10.5173/ceju.2014.04.art24
- Buckley, J. C., & McAninch, J. W. (2006). Use of ultrasonography for the diagnosis of testicular injuries in blunt scrotal trauma. Journal of Urology, 175(1). https://doi.org/10.1016/S0022-5347(05)00048-0
- Delgado-Muñoz, P., Santos, M., Saldana, A., Figueroa-Diaz, L. C., & Rodriguez-Mojica, W. (2021). Status post vasectomy: What sonographic changes to expect [Conference poster]. European Congress of Radiology 2021. European Society of Radiology. https://dx.doi.org/10.26044/ecr2021/C-11971
- Fenton, L. Z., Karakas, S. P., Baskin, L., & Campbell, J. B. (2016). Sonography of pediatric blunt scrotal trauma: what the pediatric urologist wants to know. In Pediatric Radiology (Vol. 46, Issue 7). https://doi.org/10.1007/s00247-016-3600-4
- Guichard, G., el Ammari, J., del Coro, C., Cellarier, D., Loock, P. Y., Chabannes, E., Bernardini, S., Bittard, H., & Kleinclauss, F. (2008). Accuracy of Ultrasonography in Diagnosis of Testicular Rupture After Blunt Scrotal Trauma. Urology, 71(1). https://doi.org/10.1016/j.urology.2007.09.014
- Heller, M. T., Fargiano, A., Rudzinski, S., & Johnson, N. (2010). Acute scrotal ultrasound: A practical guide. In Critical Ultrasound Journal (Vol. 2, Issue 2). https://doi.org/10.1007/s13089-010-0043-2
- Hwang, J., & Alexander, L. F. (2023). Bilateral Germ Cell Neoplasia In Situ with Left Testicular Seminoma. Applied Radiology, 52(5). https://doi.org/10.37549/ar2922
- Mandava, A., Koppula, V., Yalamanchili, R., Yadav, D., & Juluri, R. (2020). Ultrasound imaging of acute scrotum: Pictorial review with etiological correlation. The ASEAN Journal of Radiology, 21(2). https://doi.org/10.46475/aseanjr.v21i2.86
- Mcdonald, M. W., Reed, A. B., Tran, P. T., & Evans, L. A. (2012). Testicular tumor ultrasound characteristics and association with histopathology. Urologia Internationalis, 89(2). https://doi.org/10.1159/000338771
- Nakayama, A., Ide, H., Osaka, A., Inoue, Y., Shimomura, Y., Iwahata, T., Kobori, Y., Saito, K., Soh, S., & Okada, H. (2020). The Diagnostic Accuracy of Testicular Torsion by Doctors on Duty Using Sonographic Evaluation with Color Doppler. American Journal of Men’s Health, 14(5). https://doi.org/10.1177/1557988320953003
- Nikolic, O., Mrdanin, T., Basta Nikolic, M., Stojanovic, S., Petrovic, K., Vucaj Cirilovic, V., Govorcin, M., & Senicar, S. (2012). Ultrasonography of acute scrotum [Conference poster]. European Congress of Radiology (ECR) 2012. European Society of Radiology. https://doi.org/10.1594/ecr2012/C-0331
- Ota, K., Fukui, K., Oba, K., Shimoda, A., Oka, M., Ota, K., Sakaue, M., & Takasu, A. (2019). The role of ultrasound imaging in adult patients with testicular torsion: a systematic review and meta-analysis. In Journal of Medical Ultrasonics (Vol. 46, Issue 3). https://doi.org/10.1007/s10396-019-00937-3
- Radiopaedia contributors. (n.d.). Spermatocele [Radiology case]. Radiopaedia.org. https://radiopaedia.org/cases/spermatocele-1
- Rao, M. S., & Arjun, K. (2012). Sonography of scrotal trauma. Indian Journal of Radiology and Imaging, 22(4). https://doi.org/10.4103/0971-3026.111482
- Trojian, T. H., Lishnak, T. S., & Heiman, D. (2009). Epididymitis and orchitis: An overview. In American Family Physician (Vol. 79, Issue 7).
- Tyloch, J. F., & Wieczorek, A. P. (2016). Standards for scrotal ultrasonography. Journal of Ultrasonography, 16(67).
- Venyo, A. K. G. (2024). Spermatocele: A Review and Update. International Journal of Clinical Therapeutics, 3(6).
- Zitek, T., Ahmed, O., Lim, C., Carodine, R., & Martin, K. (2020). Assessing the utility of ultrasound and urinalysis for patients with possible epididymo-orchitis – a retrospective study. Open Access Emergency Medicine, 12. https://doi.org/10.2147/OAEM.S234413
