Definition: Fracture at the proximal articular surface of the radius within the elbow joint
Epidemiology
- Most common elbow injury among adults (50% among adults, 20% overall) (Schwartz 2008)
- One of the most commonly missed injuries in the ED and on radiographs
- One study showing that up to 12% of elbow fractures were missed on initial radiographic interpretation in the ED (Freed 1984)
Mechanism
- Typically result from indirect trauma: fall on outstretched hand (FOOSH) of an abducted arm with minimal to moderate flexion of the elbow joint
- Direct blows to the elbow can cause radial head fractures, however they are less common
Physical Exam
- Swelling of the elbow joint
- Tenderness with palpation on the lateral surface of the elbow
- Pain with flexion/extension of the elbow
- Inability or difficulty with pronation or supination at the elbow
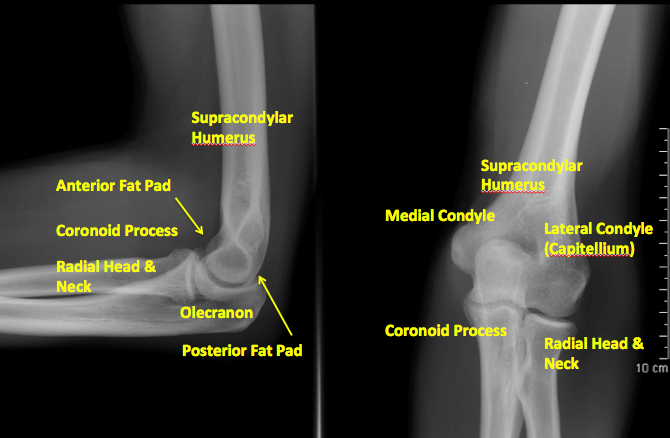
X-ray of Normal Elbow Anatomy
Radiographs
- Adequate X-ray include two views
- AP view: Elbow fully extended and no overlap of the radius and ulna
- Lateral film where the elbow is flexed at 90 degrees
- Greenspan View
- An oblique/radiocapitellar view
- Can reveal an intraarticular nondisplaced radial head fracture.
- Often not required as doesn’t change ED management
- A – Alignment
- Anterior humeral line
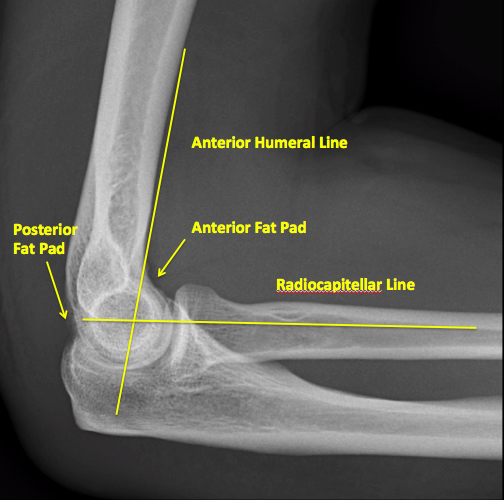
X-ray of Normal Elbow Alignment
- Drawn down the anterior aspect of the humerus and should intersect with the middle third of the capitellum.
- Posterior displacement of the capitellum should raise suspicion for a supracondylar fracture.
- Radiocapitellar line
- Aligned in both AP and lateral views.
- A disruption along this line should raise suspicion for a lateral condyle fracture or a radial head/elbow dislocation.
- Anterior humeral line
- B – Bones: Gross examination of the bones will show any obvious fractures of radius, ulna, humerus or olecranon.
- C – Cartilage (Soft Tissue).
- The elbow’s synovial joint capsule has a volume of approximately 25-30 cc
- Fat pads: Synovial joint is surrounded by a deposit of fat within the coronoid and olecranon fossae
- Anterior fat pad: Small and normall visible on a lateral XRay
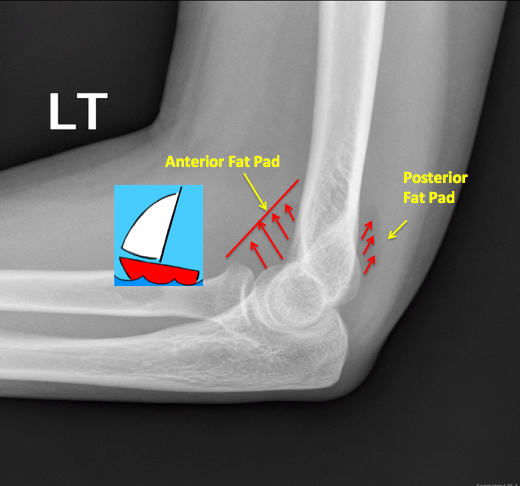
X-ray Elbow: Sail Sign
- Abnormal fat pad: an elevated anterior fat pad or any visualized posterior fat pad is indicitive of an elbow injury.
- Sail sign: An elevated, sharply demarcated anterior fat pad. It is often the only radiographic signs for a radial head injury.
- Anterior fat pad: Small and normall visible on a lateral XRay
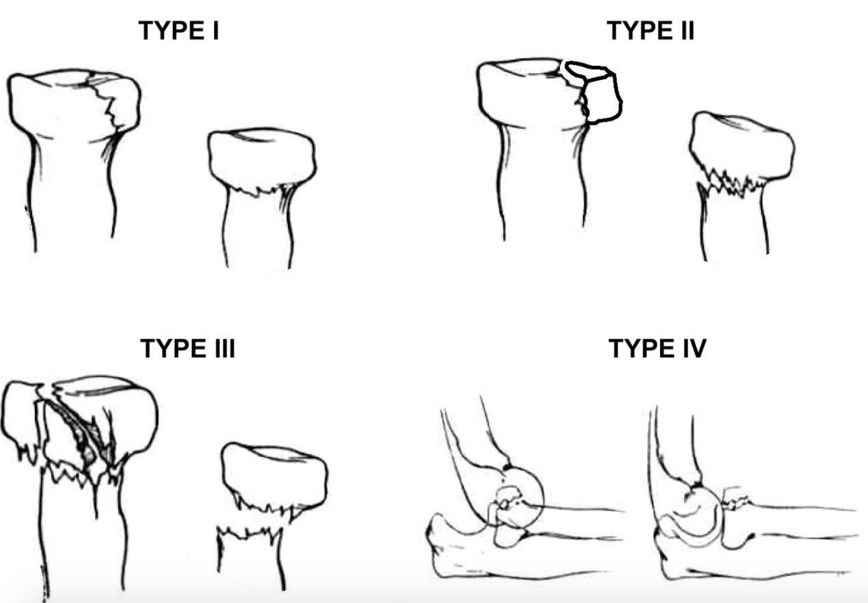
Mason Classification of Radial Head Fractures
Mason Classification
- Type I – Minimally displaced, no mechanical block to rotation, intraarticular displacement < 2 mm
- Type II – Displaced fracture > 2 mm or angulated, possible mechanical block to forearm rotation
- Type III – Comminuted and displaced fracture, mechanical block to motion
- Type IV – Radial head fracture with elbow dislocation
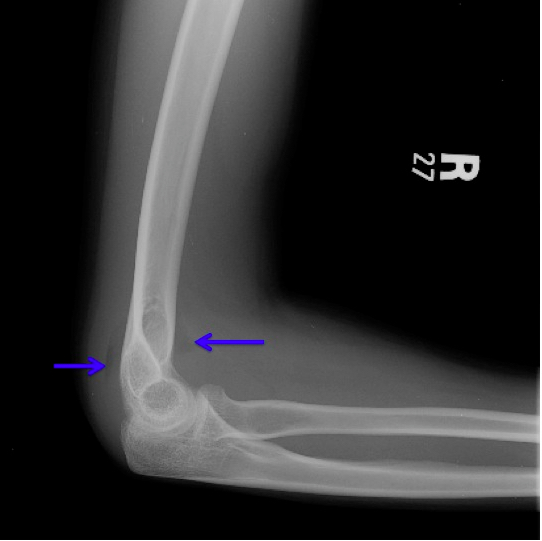
Radial Head Fracture with Sail Sign and Posterior Fat Pad (http://ortho-teaching.feinberg.northwestern.edu/cases/elbow/case2/case16additionalimages.html)
Emergency Management
- Minimally displaced radial head fractures (Mason Type I)
- Conservative management with sling placement and early mobilization
- If fracture suspected based on examination but not seen on X-ray, conservative management with sling appropriate as well
- Refer for outpatient orthopedic follow up
- Radial head fractures with mechanical block (Mason Type II) or multiple comminuted fractures (Mason Type III) should have urgent orthopaedic consultation for possible ORIF, fragment excision, or radial head replacement (Jones 2015)
- There is inconclusive evidence supporting the use of elbow joint aspiration for the treatment of immediate and long term pain and function (Foocharoen 2014)
Take Home Points
- Radial Head Fractures are one of the most commonly missed fractures of the upper extremity. An understanding of the physical examination and radiograph findings is essential.
- Remember the A-B-C (Alignment, Bones, Cartilage/soft tissue) approach to adult elbow radiographs.
- It is appropriate to discharge patients with nondisplaced radial head fractures in a sling with recommendations for early mobilization and orthopedic follow up.
Read More
Radiopaedia: Sail Sign
References
Freed H, Shields N. Most Frequently Overlooked Radiographically Apparent Fractures in a Teaching Hospital Emergency Department. Ann Emerg Med1984; 13(10): 900-904. PMID: 6476514
Jones T. (2015, December 7). Radial Head Fractures [Ortho Bullets] Retrieved from http://www.orthobullets.com/trauma/1019/radial-head-fractures
Foocharoen T et al. Aspiration of the elbow joint for treating radial fractures.Cochrane Database Syst Rev 2014 PMID: 25416525
Weerakkody Y Hartley L et al. Adult elbow radiograph (an approach) [Radiopaedia] Retrieved from http://radiopaedia.org/articles/adult-elbow-radiograph-an-approach
Schwartz, D “Upper Extremity: Patient 1” Emergency Radiology: Case Studies, McGraw-Hill, 2008 pg 235-240
